Download
1 / 31
550 likes | 3.26k Views
Parenteral Nutrition. NFSC 370 McCafferty. Definition. TPN = Total Parenteral Nutrition Provision of nutrients intravenously Central Peripheral For patients who are already malnourished or have the potential for developing malnutrition and who are not candidates for enteral nutrition.

E N D
Parenteral Nutrition NFSC 370 McCafferty
Definition • TPN = Total Parenteral Nutrition • Provision of nutrients intravenously • Central • Peripheral • For patients who are already malnourished or have the potential for developing malnutrition and who are not candidates for enteral nutrition
Advantage: Potentially life-saving when GI tract cannot be used or when oral/parenteral nutrition cannot meet nutrient requirements of patient.
Disadvantages: • Costly • Long term risk of liver dysfunction, kidney and bone disease, and nutrient deficiencies • .
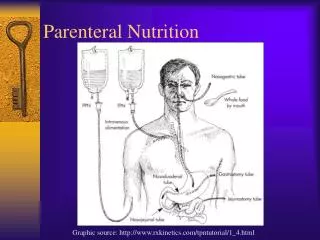
Routes for Parenteral NutritionCentral Venous Access Central Parenteral Nutrition (CPN): Central Venous Access • Utilization of large central veins for the administration of a patient’s complete nutrient needs • Preferred Route • . • Can deliver daily requirement for kcals, protein, micronutrients in concentrated volumes
Routes for Parenteral NutritionCentral Venous Access • PICC Line • Peripherally inserted central catheter • Benefits • Access to central vein • Can accommodate hypertonic fluids • Lower risk of phlebitis than PPN • Easier to insert than central line
Indications for TPN • NPO for extended period • Enteral nutrition support projected to be inadequate for • Severe acute pancreatitis • High output enterocutaneous fistulas
B. Contraindications 1. 2.
TPN Solution • Carbohydrate: Dextrose • Most common concentrations: 50% and 70% • Protein: AAs • Most common concentrations: 8.5% and 15%. • Lipid: IV emulsion • 10% solution = • 20% solution = • Concentrated source of kcals
Lipid, cont. • Helps minimize hyperglycemia • Helps prevent respiratory acidosis (in respiratory failure) • Need at least 10% of kcals from lipid to prevent EFA deficiency • Excessive lipid administration may suppress immune fx. • Often hung separately • Admixtures (3:1) becoming more common • Potential source of vit. K: potential problem if anticoagulants used
4. Vitamins Daily MV in formula is standard 5. Electrolytes • Start with standard amounts • Adjust as needed 6. Common Medications • Insulin • H2 antagonists • heparin
Peripheral Parenteral Nutrition (PPN) Utilization of peripheral veins for the administration of nutrients A. Indications for use: • PN necessary but no access to central vein 3. Malnourished patients with frequent NPO for procedures/tests
B. Contraindications: • Patient can be fed enterally • Pt. has weak peripheral veins C. Limitations • Peripheral site more prone to inflammation/infection • Catheter may need to be repeatedly inserted Poor choice for long-term nutrition
D. PPN Solution 1. Typically delivers 1400-2500 kcals/day 2. Carbohydrate: Dextrose (glucose) 3. Protein: AAs 4. Lipid: IV lipid emulsion a. Concentrated source of kcals b. Isotonic c. Administered every day to protect vein
Intravenous Solutions Abbreviations: D: dextrose W: water NS: normal saline (0.9% sodium chloride solution) D5W: D10W: D50W: D70W:
Calculations • Dextrose = • AA = • Lipid • 10% lipid provides • 20% lipid provides • Lipid can be infused separately or with dextrose and amino acid (admixture)
TPN Orders – Several ways they can be written. Examples: • Per liter • Example: 500 ml 70% dextrose, 500 ml 15% AA @ 50 ml per hour, plus 250 ml 20% lipid/d • Final concentration • Example: 20% dextrose, 6% AA at 85 ml/hr plus 500 ml 10% lipid/d • Per Day: • 960ml 8.5% Aas, 960ml D50W at 80ml/hr, plus 250 ml 20% lipids q day
Example1: Figure out total kcalories and protein gramsper day from this per liter order: 500 ml 8.5% AA/L 500 ml D50W/L to be run@83ml/hr. plus 500ml 10% lipid = 1 liter ‘admixture’ In this example, lipids are hung separately
Protein Grams (per 500 mL): Kcalories (per L):
Example 2: Calculate total kcals and protein grams provided in this per-day formula 960ml 8.5% AAs 960ml D50W to run @ 80ml/hr (X 24h = 1920ml) plus 250 ml 20% lipids q day
D50W: 8.5% AAs: Lipids:
TPN Administration • Rate • Start slowly, especially w/dextrose. Allows blood to adapt to increased glucose/osmolality • Infusion pump is used to ensure proper rate. • Example: Start at 40ml/hr x 24hr. Then progress to 80ml/hr x 24h (equivalent to increasing TPN by 1 liter per day), etc. until goal rate has been reached or patient intolerance is noted.
a. If rate is increased too quickly, hyperglycemia may result b. Monitor tolerance: electrolytes, blood glucose, triglycerides, ammonia, etc. 4. Introduce lipids gradually to avoid adverse reactions (fever, chills, backache, chest pain, allergic reactions, palpitations, rapid breathing, wheezing, cyanosis, nausea, and unpleasant taste in the mouth) 5. When pt. is taken off TPN, rate must be tapered off gradually to prevent hypoglycemia. 6. ( TPN by ½ X 2 hrs, then DC – usually sufficient to prevent hypoglycemia) 7. PPN doesn’t need to be tapered off (uses more dilute solution w/less dextrose)
Cyclic Infusion • TPN infused at a constant rate for only <24 hours/day (e.g. 12-14hr overnight) • Allows more freedom/normal daytime activity • Can be used to reverse fatty liver resulting from continuous infusion (Chronically high insulin levels may inhibit fat mobilization fatty liver) • Fewer kcals may be necessary to maintain N balance (body fat better mobilized for energy) • Requires higher infusion rate: not all patients can tolerate it.
Potential TPN Complications • Catheter or Care-Related Complications: • Fluid in the chest (hydrothorax) • Air or gas in the chest (pneumothorax) • Blood in the chest (hemothorax) • Sepsis • Blood clot (thrombosis) • Infusion pump malfunctions • Myocardial or arterial puncture
B. Metabolic or Nutrition-related Complications • Hyperglycemia/Hypoglycemia • Dehydration/Fluid overload • Electrolyte imbalances • Hyperammonemia • Acid-base imbalance • Fatty liver • Bone demineralization
Transitional Feedings -- moving from parenteral to enteral nutrition • Begin oral diet while tapering off TPN
B. Tube feeding while tapering off TPN • Rate of TF gradually increases as TPN rate decreases • Remember that long term TPN without enteral nutrients atrophy of intestinal villi C. Discontinue TPN when oral/enteral intake provides • Consider possible apprehension to begin oral intake • Poor appetite possible at first • Team members should provide support and reassurance