Download
1 / 31
310 likes | 596 Views
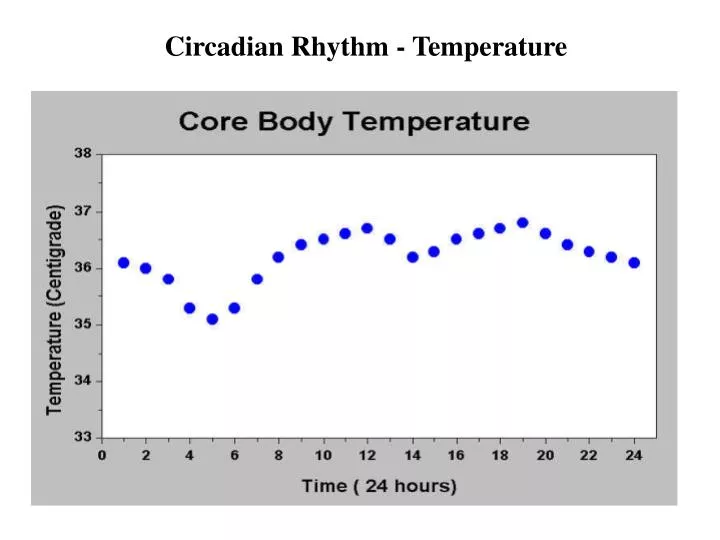
Circadian Rhythm - Temperature. Very drowsy and would love a little nap Wide Awake and rearing to go Asleep – do not disturb. BLUE YELLOW WHITE. QUESTION “How are you feeling?”. NOW!. A Child with Failure to Thrive . Colin Wallis Respiratory Unit Great Ormond Street Hospital.

E N D
Very drowsy and would love a little nap Wide Awake and rearing to go Asleep – do not disturb BLUE YELLOW WHITE QUESTION“How are you feeling?” NOW!
A Child with Failure to Thrive Colin Wallis Respiratory Unit Great Ormond Street Hospital
FTND - asymmetrical IUGR • Birth weight 1.9 kgs < 0.4th centile • Length 42 cms < 0.4th centile • OFC 33.2cms > 25th centile • Ventilated for 3 days and discharged home in air at 14 days
Referred to GOSH for further investigations Readmitted 10 days later to local hospital for poor weight gain and intermittent diarrhoea • FBC and serum biochemistry were normal • TORCH screen - negative • Some episodes of fasting hypoglycaemia • No catch up growth despite adequate caloric intake via • NGT feeds
Coeliac screen Endoscopy Sweat test BLUE YELLOW WHITE QUESTION“What test is likely to be most useful?” NOW!
Coeliac screen – negative GI endoscopy and colonoscopy were normal including histology of large bowel Sweat test - positive Na 60 mmol/l ; Cl 111 mmol/l
Usual multivitamin supplementation and prophylactic antibiotics • Adequate caloric intake with creon supplementation • Overnight NGT and top-up feeds A diagnosis of Cystic Fibrosis was made • CF genotype - R1162X/R1162X • Stool elastase - < 15 mcg/g {>200mcg} • Positive sweat test
Remove ng tube and monitor weight gain Insert gastrostomy for long term feeding Consider diabetes BLUE YELLOW WHITE QUESTION“What next?” NOW!
Ng tube was removed with very poor feeding and further loss of weight • No evidence of diabetes • Gastrostomy inserted at age 3 years
…… and so over the next 2 years …………. • Overnight feeds with additional boluses during the day • Persisting FTT with weight and height well below 0.4th centile and intermittent diarrhoea • No chest infections - only growth of Ps. aeruginosa at 4 years of age At 5 years : Weight - 12 kgs <0.4th centile Height - 95 cms <0.4th centile FVC 117% of predicted FEV1 117% of predicted
Yes – Endocrine review Yes – Gastroenterology review No – This needs psychosocial input BLUE YELLOW WHITE QUESTION“Does she deserve further investigation?” NOW!
For those of you who voted Endocrine: • Skeletal survey at 5 yrs - delayed bone age 2.5 yrs • Normal amino acid profile • Growth hormone assay - normal • Normal IGF1 & IGFBP-3 • Normal thyroid function tests • Normal cortisol , insulin and glucose levels • Normal NEFA and BOHB (rules out fatty acid oxidation defects)
For those of you who voted Gastroenterology: • Stool elastase still very low • pH study normal - pH study - 0.5% reflux • Repeat upper GI biopsies suggestive of duodenitis with mucosal eosinophilic infiltrate • Started on MCT feeds (peptamen) & PO Sodium cromoglycate • Improved stool consistency with occasional diarrhoea • Introduction of dairy free diet …. And the failure to thrive persisted….
For those of you who voted Psychosocial: • Psycho-social issues - Parental disharmony • Father blamed mother for the CF in their child – refused to accept that he had a genetic role in the condition • Suggested genetics counselling
Full term gestation • Birth weight & length <2SD below mean • Postnatal growth <2SD below mean for height & weight • Triangular face (Craniofacial disproportion) • Down turned corners of mouth • Clinodactyly, and usually shorter digit than normal • Scaphocephaly • Hypoplastic mandible and small, crowded teeth • Low set, small, or prominent ears • Delays in bone age and poor muscle tone Genetics review Phenotypically resembles Russell Silver Syndrome
Common traits: • Body asymmetry • Growth hormone deficiency • Hypoglycaemia in infancy and early childhood • Late closure of the fontanelle • Hypoplastic mandible and small, crowded teeth • Low set, small, or prominent ears • Delays in bone age and poor muscle tone • Thin upper lip with down turned corners of mouth • Syndactyly of toes • Developmental delay Phenotypically resembles Russell Silver Syndrome Are you sure this is CF?
Mum – carrier for R1162X 32 31 Dad – not a carrier 9 6 3 46XX, homozygous for R1162X mutation
Glad I don’t have to explain non-paternity to this family Ask genetics to approach the family I’m staying well out of this BLUE YELLOW WHITE QUESTION “How are you feeling now?”
What is Uniparental Disomy? • UPD is the inheritance of both homologues of a chromosome pair from only one parent. • In 2/3 of cases the UPD is of maternal origin. • UPD can result in: • the appearance of recessive disorders depending on the chr. • developmental and growth abnormalities (due to imprinting) • no apparent impact on the health of the individual. Mum – carrier for R1162X 32 31 Dad – not a carrier Dad is the father 9 6 3 46XX, homozygous for R1162X mutation Child has uniparental disomy
Genetics of Russell Silver Syndrome • 10% of cases of RSS have maternal UPD7 • Genetically heterogeneous • 80% cases sporadic • (AD/AR/XL) • RSS caused by matUPD7 gives a milder phenotype, but the feeding problems are more severe.
Normal Meiosis • Start with a cell with 46 chromosomes • Sister Chromatid formation • Meiosis I: the homologous pairs separate into two new daughter cells. • Meiosis II: the replicated pair of sister chromatids separates into two new daughter cells.
Meiotic Errors Meiosis I error Meiosis IIerror homologous pairs both travel into the same daughter cell. chromatids will not separate and thus travel into the same daughter cell.
By Trisomic rescue By Monosomic resuce Gamete complementation Don’t know what you’re on about BLUE YELLOW WHITE Hold up nothing QUESTION“How does UPD occur?” NOW!
How does UPD occur ? : CF Mutation on 7q31.2 Trisomic Rescue Fertilisation following Meiosis II error Monosomic Rescue Fertilisation following Meiosis II error Gamete Complementation
How does UPD cause CF? • Patient AA is homozygous for the R1162X (arginine-stop) mutation as she has inherited both chromosome 7’s from her mum. • Children with this form of CF do not have normal AR risks for future pregnancies – recurrence risk very low • Gasparini et al looked at the clinical course of 9 patients homozygous for this mutation: • Lung disease was mild-moderate • Higher rates of pseudomonas colonisation • Higher rates of ABPA • Pancreatic insufficiency was severe • And our patient also has Russell Silver syndrome
Lessons and questions from an interesting case • UPD is a rare but possible cause of autosomal recessive disorders • We should be suspicious of FTT in CF with Russell Silver phenotype – but should we screen CF patients with unusual growth retardation for matUPD7 ? • Should we be doing parental tests on all homozygous CF children? • Testing DNA from parents and child can potentially uncover nonpaternity. Should this be discussed as part of informed consent ? • Do these findings introduce new treatment options? • Growth hormone therapy • Nebulised or systemic gentamicin • Be aware