Download
1 / 18
190 likes | 368 Views
CTOP Retreat 2014 Esophageal Cancer Pathway. May 23, 2014. Introduction. Esophageal cancer is the 7 th leading cause of cancer death. Incidence of esophageal cancer has increased faster than any other solid tumor.

E N D
CTOP Retreat 2014Esophageal Cancer Pathway May 23, 2014
Introduction • Esophageal cancer is the 7th leading cause of cancer death. • Incidence of esophageal cancer has increased faster than any other solid tumor. • Despite advances in diagnosis, staging and treatment, the overall 5-year survival ranges from 15-30%. • Surgery for esophageal cancer has a routine complication rate of 50-75%.
In these discouraging numbers lies an opportunity to have a meaningful and measurable impact on patient care.
Mission: To provide a Dartmouth standard of care that surpasses current national standards Vision: Through the development of evidence-based clinical care pathways, we create a program to provide the highest quality of care for esophageal cancer patients Aims: • To assess current needs of patients and resources • To build a team of providers invested in a shared clinical pathway • To map the flow of patients through treatment of esophageal cancer • To optimize efficiency and evidence-based medicine • To track process and outcomes
Aim 1: To assess current needs of patients and resources • List every contact with a DHMC service a patient with esophageal cancer may have • List all necessary studies (pathology, radiology, endoscopy) a patient may need, and the optimal order of events • Mailed questionnaire to patients. • “What did we do well?” • “Where could we improve?” • Reunion of past patients
Aim 2: To build a team of providers invested in a shared clinical pathway Secretarial lead Nurse navigator Physician lead Surgery-anesthesia Quality-Electronic Medical Record
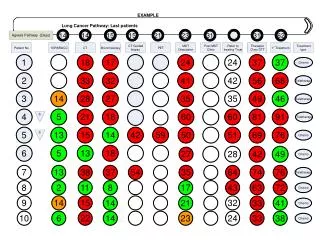
Aim 3: To map the flow of patients through treatment of esophageal cancer
Aim 4: To optimize efficiency and evidence-based medicine • Identify optimal, evidence-based practices • Identify opportunities to • Educate patients • Educate providers • Reorganize current resources
Aim 5: To track process and outcomes • Retrospective chart review of pathway patients • Compare to previous consecutive esophagectomy patients
Pathway vs. Controls • No demographic differences
Immeasurable Benefits • Patient connection with providers • Providers working as a team with equal voice • Identify deficiencies
Limitations • Few patients • Maintenance of pathway • Resources
Future Directions • Pathway integrated with database • Pathway manager?
Thank You Questions?
To personalize the experience of each patient treated for esophageal cancer at DHMC-NCCC • Patient Binder • Patient Video • Shared Decision-making
Learning about esophageal cancer • The esophagus is a muscular tube connecting the mouth and the back of the throat (pharynx) to the stomach. • Normal cells of the esophagus grow and divide to replace old or damaged cells • Sometimes this process goes wrong. New cells form when the body does not need them or damaged cells do not die as they should. The buildup of extra cells forms a mass of tissue called a tumor • Esophageal cancer begins in the inner layer of the esophagus. Over time, the cancer may • invade more deeply into the esophagus • Spread to nearby lymph nodes* • Spread to other parts of the body *Lymph nodes normally act as filters. They filter out infection and cancer. Often, esophageal cancer will spread to lymph nodes before spreading to other parts of the body Revised from National Cancer Institute http://www.cancer.gov/cancertopics/wyntk/esophagus