Download
1 / 24
250 likes | 529 Views
Antipsychotic Agents. MS2 Lecture Sean Conrin MD. Contents. Psychosis and Schizophrenia The Framework Neuroanatomy Circuits Important Neurotransmitters Anti-psychotics Dopamine Hypothesis Typical Antipsychotics Atypical Antipsychotics Side Effects. Psychosis – What is it?.

E N D
Antipsychotic Agents MS2 Lecture Sean Conrin MD
Contents • Psychosis and Schizophrenia • The Framework • Neuroanatomy • Circuits • Important Neurotransmitters • Anti-psychotics • Dopamine Hypothesis • Typical Antipsychotics • Atypical Antipsychotics • Side Effects
Psychosis – What is it? • 1. Being “out of touch” with reality • 2. Alternate definition similar to similar symptoms listed as part of diagnostic criteria. • Hallucinations (lack of insight) • Delusions • Disorganized/catatonic behavior • Negative symptoms (?)
Psychosis is like a fever!(It can happen for a number of reasons) Primary Psychotic Illness Psychosis Primary Mood Disorder Medical and Substance
DSM V - Schizophrenia • A – Two or more for significant portion of a 1-month period. One must be of the first three • 1. Delusions • 2. Hallucinations • 3. Disorganized Speech • 4. Grossly disorganized/catatonic behavior • 5. Negative symptoms • B – During this time, impairment in functioning in at least one domain
DSM V - Schizophrenia • C – Continuous signs of disturbance for at least 6 months (w/ one month of full criteria A symptoms) in the form of attenuated A, prodromal or negative symptoms. • D – Not part of another illness • E – No due to a substance or medical condition • F – If autism or communication disorder, only diagnose if prominent delusions or hallucinations are present for one month • Specifications for episode pattern • Specifications for severity (1-5 scale) of each symptom domain
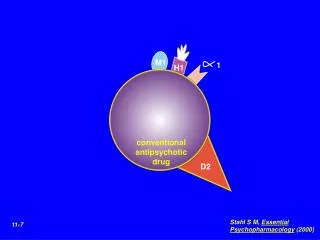
Dopamine Hypothesis • In 1950’s discovery that Chlorpromazine administration led to less response to adverse stimuli in rats. - Initially thought it was H1 effects - Methylene Blue is also a phenothiazine • Gave it to humans and saw that it worked well • 100 million have been treated at least (same scale as antibiotics) • Learned it’s main effect was on dopamine • Affects all dopamine pathways (good and bad)
The Brainstem • Midbrain • “Meso” • Substantia-Nigra • Dopamine • Pons • Contains Locus Coeruleus (NE) • Medulla • Pyramids (EPS!) • Raph Nuclei • Located throughout brainstem • Serotonin
The Brain Has a “Few” Connections • These are the main connections involving dopamine • Limbic System • Cortex • Tubero
Mesocortical (cognition) Mesolimbic (hallucinations) Nigrostriatal (movement) Tuberoinfundibular(prolactin)
Typicals • High Potency - Haldol - Fluphenazine - Prochlorperazine • Low Potency - Chlorpromazine - Thioridazine (Retinitis Pigmentosa – buzzword alert) Atypicals • Risperdal (functions like typical at higher doses) • Quetiapine (titrate so pt doesn’t fall) • Aripiprizole (partial D2 antag) • Ziprasidone (QT prolong) • Lurasidone (new) • Iloperidone (new – titrate to avoid falls) • Asenapine (new – dissolved under tongue) Atypical, Atypical • Clozapine - WBC/ANC monitoring for risk of agranulocytosis - Indicated for suicidality in schizophrenia - Most effective
Atypical Antipsychotic Release Dates • Clozapine 1989 • Risperidone 1993 • Olanzapine 1996 • Quetiapine 1997 • Ziprasidone 2001 • Aripiprazole 2002 • Asenapine 2009 • Iloperidone 2009 • Lurasidone 2010
Monthly Cost of Antipsychotic Medications (From Consumer Reports 2009)
Typical vs Atypical • Refers to extrapyramidal symptoms - Old vs New - Cheap vs Expensive • EPS (1st gen > 2nd gen) - Parkonsonism - Tardive Dyskinesia - Akathisia - Dystonic Reaction • Cardiometabolic (2nd gen > 1st gen) - Weight - Glucose - Lipids - Cardiovascular
High vs Low Potency • Potency - Refers to potency at D receptors - Think ETOH (wine < potent than rum so you need less rum to have the same effect) • High Potency (2-20mg) - More likely to cause EPS • Low Potency (100’s-2,000mg) - More H1/Ach/Alpha blockade • Be able to identify High vs Low based on milligrams and say how they differ!
Dystonic Reactions • Nigrostriatal– D2 blockade leads to increased ACH. This causes inhibition of spontaneous movement and parkinson like symptoms. • Dystonias + parkinsonism • Benztropine – (cogentin) is an anti-cholinergic, this realigns the balance and decreases EPS • High vs Low Potency – Low potency drugs such as thioridazinehave significant anticholinergic properties. • Compared to high potency, like haloperidol cause less eps
Tardive Dyskinesia • Tardive dyskinesia – prolonged blockade of D2 receptors leads to upregulation of D2 receptors. • Causes hyperexcitability: writhing tongue and hand movements, • 5% per year on typicals • NOT FIXED BY BENZTROPINE! • AIMS Antipsychotic
Akathisia • Inner sense of restlessness • Can lead to increased violence or suicide • Can be treated with propranolol, some give benzos or anticholinergics (not as effective) • Often misclassified, especially in antidepressant trials and can be hard to recognize in DD or nonverbal patients. • Barnes Akathisia Scale
Anticholinergic Effects • “Red as a beet” (loss of sweating so vasodilation occurs) • “Dry as a bone” (loss of sweating) • “Hot as a hare” (loss of sweating) • “Blind as a bat” (pupillary constriction and effective accommodation blocked – blurry vision) • “mad as a hatter” (delirium/hallucinations) • “Full as a flask”
Atypicals • Huh? – Basically low eps, and good(?) for negative symptoms • So? – Four proposed mechanisms • Serotonin/dopamine antagonism • D2 antagonism w/ rapid disassociation • D2 partial agonists • Serotonin partial agonists
So What’s the Deal? • Weight Gain – antipsychotic drugs act on hypothalamus and stimulate appetite. Antagonism of alpha adrenergic, dopamine, histamine 1, glutamate, muscarinic type 1, 5HT2A and 5HT2C • Some evidence regarding concurrent H1 and 5HT2C antagonism – Especially Problematic • Also – 2nd gens might work on peptides galanin, neuropeptide U and leptin
Atypical Antipsychotics and Weight Gain • 10 weeks on drug • Ziprasidone 0.09 pounds • Haloperidol 1.1 pounds • Aripiprazole 1.6 pounds • Risperidone 4.4 pounds • Chlorpromazine 4.7 pounds • Olanzapine 7.8 pounds • Thioridazine 7.8 pounds • Clozapine 8.9 pounds