Download
1 / 26
340 likes | 629 Views
Re-establishing Neuromuscular Control. Why is it critical to the rehabilitation process?. Refocuses the athlete’s awareness of peripheral sensation & guides them into more coordinated motor strategies Required to: Protect joints from excessive strain

E N D
Why is it critical to the rehabilitation process? • Refocuses the athlete’s awareness of peripheral sensation & guides them into more coordinated motor strategies • Required to: • Protect joints from excessive strain • Provide prophylactic mechanism to recurrent injury • Complements traditional components of rehabilitation • We rely on sensory information from the periphery from our visual, vestibular, & somatosensory systems.
Primary role of articular structures • Stabilize & guide body segments • Provide mechanical restraint to abnormal joint motion • Dynamic restraint system • Capsuloligamentous tissue & musculotendon receptor sensory role • Detect joint motion & position • Detect changes in muscle length • Implicated in regulating muscle stiffness prior to loading • Injury results in damage to microscopic nerves associated with peripheral mechanoreceptors • Disrupts sensory feedback • Alters reflexive joint stabilization & neuromuscular coordination
Four critical elements of neuromuscular control in rehab • Joint sensation (position, motion, force) • Dynamic stability • Preparatory & reactive muscle characteristics • Conscious & unconscious functional motor patterns • Rehabilitation should address feedback systems • Preparatory (feed-forward) • Reactive (feed-back) • Muscle sense is divided into 4 sensory functions: • Sensation of passive movement • Sensation of active movement • Sensation of position • Sensations of heaviness & resistance
What is neuromuscular control? • Signal transmission through afferent sensory pathways • Proprioception • Conscious & unconscious appreciation of joint position • Awareness of position & movement • Any postural, positional or kinetic info provided to the CNS by sensory receptors in muscles, tendons or joints • Kinesthesia • Sensation of joint motion or acceleration • Sensation of ACTIVEmovement (contracting muscle) • Neuromuscular control • Efferent motor response to sensory information • Proprioception & kinesthesia
Motor control mechanisms • Feed-forward neuromuscular control • Planning movements based on sensory information from past experiences • Preparatory muscle activity • Operates on premise of initiating a motor response in anticipation of a load or activity • Feed-back neuromuscular control • Continuously regulates muscle activity through reflexive pathways • Reactive muscle activity • Operates directly in response to a potentially destabilizing event, using a normal reference point • Muscle stiffness • Ratio in change of force to change in length • Stiffer muscles resist stretching = more effective restraint to joint displacement • Modified by muscle activation
Activities for Inducing Adaptations • Open & closed kinetic chain activities • Balance training • Eccentric & high repetition low load exercises • Reflex facilitation • Stretch-shortening • Biofeedback training • Controlled positions of vulnerability
Physiology of Mechanoreceptors • Articular Mechanoreceptors • Specialized nerve endings that transduce mechanical tissue deformation into frequency modulated neural signals • Increased tissue deformation results in increased afferent firing rate or rise in quantity of mechanoreceptors activated • Types • Pacinian corpuscles – (Type II) sensitive to high-frequency vibration; compression sensitive • Ruffini endings – (Type I) sensitive to stretching of the joint capsule • Golgi-Mazzoni corpuscles – (Type III) sensitive to joint compression, not joint motion • Free nerve endings – (Type IV) stimulated by pain & inflammation when a joint is placed in an end position • Normally not active in normal joint movement
Articular Mechanoreceptors • Quick adapting (QA) • Cease discharging shortly after onset of stimulus • Provide conscious & unconscious kinesthetic sensation in response to joint movement/acceleration • Type II • Slow adapting (SA) • Continue to discharge as long as stimulus is present • Continuous feedback & proprioceptive information relative to joint position • Type I, III
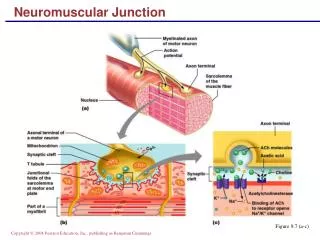
Musculotendon Mechanoreceptors • Muscle spindles – located in the muscle • Responds to stretch of a muscle • Detects length & rate of length changes • Its stimulation leads to a contraction • Transmit information via afferent nerves • Innervated by small motor fibers (gamma efferents) • Project directly on motoneurons (monosynaptic reflexes) • Stretch reflex • Stimulation results in reflex contraction • Continued stimulation (gamma motor nerves) heighten stretch sensitivity • Muscle activity mediation
Musculotendon Mechanoreceptors • Golgi Tendon Organs (GTO) – located in tendon & musculotendon junction • Detects tension within a muscle & responds to both the contraction & stretching of a muscle • Regulate muscle activity & tension • Its stimulation results in muscle relaxation • GTO’s have opposite effect of muscle spindles by producing a relaxation in the muscle being loaded
Neural Pathways of Peripheral Afferents • Encoded signals - transmitted from peripheral receptors via afferent pathways (interneurons) to CNS • Brain Stem = Balance • Primary proprioceptive correlation center • Cerebral Cortex – location of conscious movement • Monosynaptic reflex pathway - links muscle spindles directly to motor nerves • Balance • Influenced by peripheral afferent mechanism mediating joint proprioception • Partially dependent on inherent ability to integrate joint position sense, vision & vestibular apparatus with neuromuscular control
Re-establishing Neuromuscular Control • Injuries result in decreases in neuromuscular control • Pathoetiology • Injury results in deafferentation of ligament & capsular mechanoreceptors • Joint inflammation & pain compound sensory deficits • Congenital/pathological joint laxity have diminished ability to detect joint motion & position • Proprioceptive, kinesthetic deficits & mechanical instability lead to functional instability
Objectives for Neuromuscular Rehabilitation • Develop/re-establish afferent & efferent characteristics that enhance dynamic stability • Elements • Proprioceptive & kinesthetic sensation • Dynamic joint stabilization • Reactive neuromuscular control • Functional motor patterns • Afferent & Efferent Characteristics • Sensitivity of peripheral receptors • Facilitation of afferent pathways • Muscle stiffness • Onset rate & magnitude of muscle activity • Simultaneous activation of agonist/antagonist • Reflexive & discriminatory muscle activation
Neuromuscular Characteristics • Peripheral Afferent Receptors • Altered peripheral afferent information may disrupt motor control & functional stability • Repetitious athletic activity enhances proprioceptive & kinesthetic acuity = facilitated afferent pathways • Enhanced joint motion awareness improves feed-forward & feedback mechanisms • Muscle Stiffness • Significant role in preparatory & reactive dynamic restraints • Exercises that encourage muscle stiffness should be incorporated into rehabilitation programs • Eccentric exercises • Chronic overload results in connective tissue proliferation, desensitizing GTO’s & increase muscle spindle activity • Power trained vs. Endurance trained athletes • Power athlete = Faster muscle pre-activation (EMG) • Endurance athlete = Increased baseline motor tone
Reflexive Muscle Activation • Reflex latency times may be dependent on types of training (endurance vs. power) • Preparatory & reactive muscle activation might improve dynamic stability & function if muscle stiffness is enhanced in deficient joints • Decreasing electromechanical delay between joint loading & protective muscle activation can increase stability & function
Discriminate Muscle Activation • Unconscious control of muscle activity is critical in balance & coordination • May initially require conscious activation prior to unconscious control • Use of biofeedback can aid in this process • Help eliminate imbalances & re-establish preparatory & reactive muscle activity
Elements for Neuromuscular Control • Proprioception & Kinesthesia Training • Restore neurosensory properties • Enhance sensitivity of uninvolved peripheral afferents • Joint compression is believed to maximally stimulate articular receptors • Closed chain exercises through available ROM • Early repositioning tasks are critical • Conscious to unconscious joint awareness • Applying neoprene sleeve or ace wrap stimulates cutaneous receptors – additional proprioception & kinesthesia
Dynamic Stabilization • Encourage preparatory agonist/antagonist coactivation • Restores force couples & balances joint forces • Results in decreased loads on static structures • Activities that require anticipatory & reactive adjustments to imposed loads • Combination of balance & stretch shortening exercises • Encourages preparatory & reactive muscle activity • Closed chain exercises induce coactivation & compression
Reactive Neuromuscular Control • Stimulates reflex pathways • Object is to impose perturbations that stimulate reflex stabilization • Can resultin decreased response time & develop reactive strategies to unexpected joint loads • Perturbations should be unexpected in order to facilitate reflexive activity • Functional Activities • Objective is to return athlete to pre-injury activity • Involves sports specific movement patterns designed to restore functional ability • Can be utilized to assess readiness for return to play • Stresses peripheral afferents, simultaneous muscle activation, reflexive activity • Progress from conscious to unconscious • Develop functionally specific movement patterns, ultimately decreasing risk of injury
Lower Extremity Techniques • Techniques should focus on muscle groups that require attention • Progress from no weight to weight assisted • Use of closed-chain activities is encouraged • Replicates environmental demands • Plays on principles of neuromuscular control • Joint stabilization exercises • Balance & partial weight bearing activities • Progress non-weight bearing to full weight-bearing • Balance on unstable surfaces can begin once full-weight bearing
Slide board exercises • Stimulates coactivation with increasing muscle force & endurance • Stimulating dynamic stability & stiffness • Stair climbing (forward & backward) • Emphasis on eccentric strength • Biofeedback • Used to develop agonist/antagonist coactivation • Encourages voluntary muscle activation • Stretch-shortening exercises • Eccentric deceleration & explosive concentric contractions • Incorporate early in process (modified loads) • Involves preparatory & reactive muscle activity • Hopping progression • Double Single leg • Sagittal Lateral Rotational hopping • Surface modification
Rhythmic stabilization React to joint perturbations preparatory & reactive muscle activity Alterations in loads & displacement Unstable surfaces Linear & angular perturbations, altering center of gravity Facilitate reflexive activity Ball toss Disrupt concentration, induce unconscious response & reactive adaptation Trampoline Hopping Hopping & landing (double support, single support, rotation) Challenge athlete Hopping & catching Hopping & landing on varying surfaces Functional activities Restore normal gait Athlete must internalize normal kinematics (swing & stance) Utilize retro walking (hamstring activity), pool or unloading devices Cross over walking, figure 8’s, cutting, carioca, changes in speed Functional activities that simulate demands of sport
Upper Extremity Techniques • Work to maintain joint congruency & functional stability • Requires dynamic restraint via coordinated muscle activation • Injury to static stabilizers • Failure of dynamic restraint system • Could result in repetitive loads, compromising joint integrity & predisposing athlete to re-injury • Adapt lower extremity exercise for upper extremity
Muscle stiffness • Enhance using elastic resistance (focus on eccentrics) • High repetitions & low resistance • Upper extremity ergometers should be incorporated for endurance • Dynamic stabilization • Stability platforms • Push-ups, horizontal abduction, tracing circles on slide board with dominant & non-dominant arms • Plyometric exercise
Reactive Neuromuscular Exercises • Manual perturbations • Rhythmic stabilization with gradual progression • Placing joint in inherently unstable positions • Functional Training • Developing motor patterns in overhead position • Reproduce demands of activity • Emphasis on technique • Re-education of functional patterns • Speed & complexity in movement require rapid integration of sensory information