Download

1 / 35
360 likes | 532 Views
Medical Device Channels in Latin America. John Brady Mark Givens Thom Murphy Ron Sacher Mike Zajack. Agenda. Overview of current healthcare situation Overview of current distribution model Operating Considerations. Resources / 10,000 27 physicians 96 nurses Infant Mortality Rate

E N D
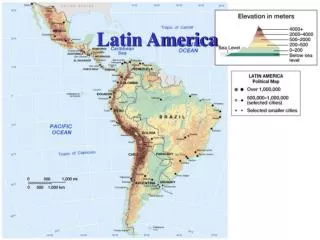
Medical Device Channels in Latin America John Brady Mark Givens Thom Murphy Ron Sacher Mike Zajack
Agenda • Overview of current healthcare situation • Overview of current distribution model • Operating Considerations
Resources / 10,000 27 physicians 96 nurses Infant Mortality Rate 7 of 1000 live births Annual Spending $4,300 per person Resources / 10,000 15 physicians 8 nurses Infant Mortality 35 of 1000 live births Annual Spending @ $200 per person How is Latin American Healthcare Different? North America Latin America Pan American Health Organization – www.paho.com
Flood, Patricia; Latin American Medical Device Regulations, MDDI – July 2000
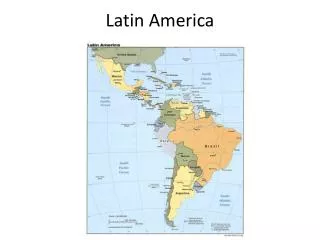
Overview of LA Healthcare Markets • Health Status • Young populations • Leading causes of death • Circulatory disease • Cancer • Respiratory Illness • Infectious and communicable diseases • Other concerns • Safe drinking water • Waste / sewage concerns • Sterilization
Healthcare System Structure • Balance of public/private development • Most are controlled by State agencies • Focus on decentralization • Largely a two-tier system: rich & poor • Two-tier again: urban vs. rural
Medical Device Market Size, 2000, (US$4.1billion) $195m $440m $2700m $90m $700m
Current Medical Device Market • Majority are imports • Specialist agents & distributors • Regional manufacturing/offices necessary • Bidding • Decentralization emphasized
Issues with Current Medical Device Market • Lack of trained personnel to run equipment or purchase appropriate equipment • High % of equipment not functioning after three years • How to transition from importer to manufacturer exporter – sustainable development
Typical Euro Models • Large Country Model • Italy, Germany, UK, France & Spain • Single Franchise sales responsibility • Franchise Director is Country Manager US Corporation US Corp Franchise Franchise owned Subsidiary in each Country
Typical Euro Models • Large Country Model • Infrastructure • Market size supports franchise based operation • Finance • Operations • Human Resources • Distribution Channel(s) • Typically Direct • Infrastructure allows more direct control of sales force • Single Franchise sales responsibility • Franchise Director is Country Manager
Typical Euro Models • Small Country Model • Czech Rep, Poland, Turkey… • Multiple Franchise sales responsibility • Multiple Franchise Directors report to CM US Corporation US Corp Franchise A US Corp Franchise B US Corp Franchise C Corporate owned Subsidiary in each Country
Typical Euro Models • Small Country Model • Infrastructure • Corporate owned subsidiary • Shared infrastructure with other franchises based on smaller market size • Distribution Channel(s) • Typically Indirect • Independent Representatives • Independent Distributors • Some Direct • Direct Rep - Sale through Local Distributor • Single Franchise sales responsibility • Franchise Director is Country Manager
Latin American Model • Corporate owned Subsidiary • Single infrastructure “umbrella” • Countries grouped into Regions • Responsible for all 5 Regions P&L Corporate Owned Latin America Subsidiary Mexico Brazil C. America Caribbean Northern Zone Ven, Col, Equa Southern Cone Chile, Arg, Urag
Latin American Model • Regional Management • Multiple franchise responsibility 1 Region – Southern Cone Regional Marketing Director Regional Sales Manager Franchise A Franchise B Franchise C
LA Model – Reg Mgt. Considerations • Distribution • Varies by Country within Region • Localized relationships necessary • Infrastructure only supports Independent Distributorships • Multiple franchise product responsibility • Ratio Management - Manage capital/inventory • Competition • Local competition knockoffs • Typically “Influential” Surgeon driven / owned • Little patent protection from Govt. – “Keep money in Country” • Pricing • Cheaper local knockoffs • rich/poor vs. high/low volume
LA Model - Reg Mgt. Considerations • Economic variability in country mix • Exchange rates • Tariff’s • Devalued currencies - export reductions • Healthcare Structure - differ among countries • Private healthcare for upper 5% only • Gov’t Subsidized • Low reimbursement - “Keep money in Country” • Slow reimbursement process – Encourages pre payment • Gov’t spending for local war Vs healthcare
LA Model – Reg Mgt. Strategy • Distribution Strategy • Invest in long term relationships • Education is key • Competition • Offer total value to customer • Surgeon education • High Quality Product • Reduce Hospital Liability • Pricing strategy • Tariffs incorporated into price • Bundling to optimize volume discounts • High volume @ lower prices or target rich @ high prices
LA Model - Reg Mgt. Strategy • Economic Stability • Budget for predicted country issues • Place manufacturing in the country • Protect outflow of capital & keep money in the country • Protection from currency exchange rates • Healthcare Strategy • Educate govt. on total healthcare costs
In addition to appendices , supporting information may be found in the slide notes provided.
Appendix 1 - Argentina • I. Argentina Medical Market • a. Intro • i. Movement to deregulate healthcare system to allow private companies to compete with trade unions. • II. Health status • a. Population primarily young. • b. Huge country – 2nd largest in South America • c. Leading cause is circulatory disease • i. Circulatory disease– 26.1% of all deaths • ii. Respiratory – 10.7% of all deaths • iii. Cerebrovascular – 8.4% • III. Structure of healthcare system in Brazil • a. Argentina spends more on healthcare than any other Latin nation • b. Complex structure – public, social insurance and private • i. Many sub entities leading to complicated administrative structure. • IV. Current distribution model • a. More lassiaz-faire than any other country. • i. Most sold through local agents and distributors. • ii. Common to buy expensive items direct from manufacturer. • iii. Distributors generally cover entire country, with network of agents throughout. • iv. Takes time to introduce new products into market: endorsements by leading doctors/hospitals are helpful. • v. Nine distributors in Argentina
Appendix 2 - Brazil • I. Brazil Medical Market • a. Intro • i. The New Constitution of 1988 created the unified health system (SUS), guaranteeing free universal healthcare to all Brazilians • ii. A two-tied system of healthcare due to extreme economic diversity in Brazil. • II. Health status • a. Population primarily young. • b. Huge country. • c. The health status of Brazil lags behind neighboring countries with similar incomes. Comparable with poorer nations like Peru. • d. 27% of population live in poverty. • e. Economic diversity leads to two disease profiles: chronic and degenerative diseases in the wealthy part, and infectious and parasitic diseases in the poorer part. • f. Sterilization is the most common form of birth control. • i. 40% of married/cohabitating women have been sterilized (27% 10 years ago). • g. Causes of death • i. Leading cause is circulatory disease • 1. Heart disease– 14.9% of all deaths • 2. Cancer – 11.9% of all deaths • 3. Infectious and parasitic – 5.2%
Appendix 2 – Brazil (cont.) • III. Structure of healthcare system in Brazil • a. SUS • i. Focused on decentralization – giving more autonomy to state and cities in planning local programs • ii. This process has been slow, marked by corruption and poor control of funds. • iii. Private insurance covers 28% of population. • 1. These companies maintain their own hospitals, medical centers, etc. • b. Localized in large population areas • IV. Current distribution model • a. Imported medical devices must meet specific requirements in order to be sold. • i. Establishment of a local manufacturing unit or local office. • ii. Establishment of a Brazilian distributor • b. Import duties and VAT taxes were abolished in 1999 to ease public health expenditures. • c. Cut tariffs up to 30% on some medical devices such as heart valves and pacemakers. • d. Public hospitals are exempt from all duties and tariffs but to import a device must prove: • i. Brazilian companies do not manufacture a similar product • ii. If it is locally manufactured, its price must be higher than the import. • e. Distribution is best done through developments with local agents or distributors. • i. On-site Brazilian reps are critical for gaining access to end-users. • ii. Personal visits to hospitals and doctors are essential. • f. In an effort to promote decentralization, federal hospitals can purchase their own medical supplies. State and locals hospitals source through the state/municpal health secretsariats. • g. 10 major distributors
Appendix 3 - Chile • I. Chile Medical Market • a. Intro • i. Imbalances remain in Chile healthcare system • ii. Standard structure of public and private medical care • II. Health status • a. Population primarily young. • b. 85% live in urban areas, 40% of population lives in Santiago. • c. Sanitation an issue in rural Chile. • i. 97% of all waste water (urban and rural) is released without being treated. • d. Causes of death • i. Circulatory disease– 27.5% of all deaths • ii. Cancer – 21.8% of all deaths • iii. Respiratory disease – 12.7% • III. Structure of healthcare system in Chile • a. Both public and private sectors regulated by Ministry of Health • b. Both sectors participate in health insurance
Appendix 3 – Chile (cont.) • IV. Current distribution model • a. Medical devices regulation in Chile is relatively new. • i. Must receive a local compliance through a government agency. • b. Best way of entry is through a local import company. • c. Market is small and personal selling/connections is important. • d. National Health Service is leading purchaser of medical devices, but hospitals are encouraged to purchase on their own. • e. Purchasing is done mostly through tender offers. • f. Importing into Chile is not difficult and there are few restrictions. • g. Chile relies highly on imported medical devices, mainly from USA. • h. 10 major distributors
Appendix 4 - Mexico • I. Mexico Medical Market • a. Intro • i. main objective of governments health care sector reform program is to address inadequacies of health care system. • b. 10m people currently no access to healthcare services and additional 20m with less than adequate access. • II. Health status • a. Causes of death • i. Seen a substantial fall in mortality from communicable diseases • ii. But a rise in mortality from chronic and degenerative diseases • 1. Heart disease– 13.8% of all deaths • 2. Cancer – 12.1% of all deaths • 3. Endocrine, nutritional, immunity disorders • III. Structure of healthcare system in Mexico • a. Comprised of 3 sectors • i. Public • ii. Social Security • 1. directly related to employment • iii. Private • b. Localized in large population areas
Appendix 4 – Mexico (cont.) • IV. Current distribution model • a. Most equipment sold through specialist agents and distributors • i. These specialize by product or brand name • b. Sales driven largely through technical advisors who call directly on hospitals and doctors. • c. Public institutions account for 80 % of market • i. Formalized bidding process • d. Private hospitals use informal process much like private US hospitals. • e. Financing is extremely important (especially in light of the Peso crisis in 1994) • i. Social Security sector has piloted a new program in which manufacturers supply devices for free in exchange for consumables contracts. • ii. NAFTA agreements exempt us from 10-20% duty charges plus 15% VAT • f. Nine major distributors, with sales ranging from $1 to $25m.
Appendix 4 – Mexico (cont.) • V. Issues with current medical device market • a. Lack of trained personnel to run equipment and purchase appropriate equipment • b. Reported 52% of imported equipment is not functioning after 3 years. • c. Reported 65-75% of medical equipment and devices needs replacing • d. Maquiladora Program - introduced in 1993 • i. Production sharing program whereby raw materials and components get imported duty-free into Mexico and assembled in Mexican medical devices • ii. Exports outpaced imports of medical devices but balance was restored in 1998. • iii. Mexican production revolves largely around consumables and low- tech devices. • iv. But 95% of high-tech equipment is still imported, mainly from USA
Appendix 5 - Peru • I. Peru Medical Market • a. Intro • i. In dire need of modernization. • ii. Health indicators are poor, with sanitation and malnutrition issues prevalent in rural parts of country. • iii. Health expenditure remains very low. • II. Health status • a. Population primarily young. • b. 74% of the population is urban. • c. Causes of death • i. Only 58% of deaths in 1999 went reported. • ii. Respiratory diseases are major recorded cause of death. • 1. Respiratory disease– 18.8% of all deaths • 2. Circulatory – 16.9% of all deaths • 3. Infectious - 8.6% • iii. Infectious is a major issue – malaria, cholera. • III. Structure of healthcare system in Peru • a. Fragmented between various government agencies • b. Small number of private hospitals • i. Based in Lima • ii. Serve a small wealthy sector • c. Localized in large population areas
Appendix 5 – Peru (cont.) • IV. Medical Device Overview • a. Most of the activity is based in Lima • b. Local agent necessary; government only issues tenders to them. • c. All purchases over US$75k must be put out to public tender. • d. 12% import customs duty and 18% sales tax. • e. 85% of market supplied through imports. • f. Huge demand for medical devices and equipment. • i. Replacement of old equipment. • ii. Providing expanded services in rural areas. • g. Equipment is largely at low/medium end of technology scale. • h. USA is leading supplier of imports to Peru.
Works Consulted • The organ shortage: a public health crisis. What are Latin American governments doing about it?, Santiago-Delpin EA, Transplant Proc, December 1997. • [The fragmentation of national health systems.], La fragmentacion de los sistemas nacionales de salud., Barillas E, Rev Panam Salud Publica, March 1997. • The transfer of vaccine technology to developing countries. The Latin American experience., Homma A; Knouss RF, Int J Technol Assess Health Care, Winter 1994. • How should resources be reallocated between physicians and nurses in Africa and Latin America?, Vargas-Lagos V, Soc Sci Med, 1991. • Distributing and transferring medical technology. A view from Latin America and the Caribbean., Pena-Mohr J, Int J Technol Assess Health Care 1987. • The medical "brain drain" and health priorities in Latin America., Horn JJ, Int J Health Serv, 1977. • DIAGNOSTICS INTELLIGENCE- Corgenix Medical Corp.: entered distribution agreements with South American companies., Chemical Business Newsbase, May 1999. • Oral Diabetes Drug to Reach Venezuela., Medical Industry Today, 1999 May. • CHILE- MEDICAL EQUIPMENT MARKET., Industry Sector Analysis, U.S. Department of Commerce., April 1999. • Merck Latin America Agrees to Market Wound Care Products., Medical Industry Today, January 1999. • St. Jude, Avecor Form Product Family for Foreign Sale., Medical Industry Today, April 1997. • TROPICAL DISEASES: Four Tropical Diseases Can Be Eliminated, WHO Says., Infectious Disease Weekly, May 1997. • Health Policy: Investing in People’s Future, The Puzzle of Latin American Economic Development [Ch. 12], Franko, Patrice M., 1999.
Works Consulted (cont.) • HNP/Poverty Thematic Group of The World Bank: Socio-Economic Differences in Health, Nutrition, and Population in Peru, Columbia, Brazil., Gwatkin, Rustein, Johnson, Pande and Wagstaff, May 2000. • MediStat Country Pofiles: Mexico, Venezuela, Peru, Argentina, Chile, Brazil, Espicom Business Intelligence, 2000-01. • Overview of Medical Equipment Market: Brazil., U.S. Foreign & Commercial Servce & U.S. Department of State, 2001. • Industrial Sector Analyses (ISA): Argentina, Chile, Mexico, U.S. Foreign & Commercial Servce & U.S. Department of State, 2001. • Emerging Market Reports: Argentina, Brazil, Chile, Mexico, HIMA, 1999.