Download

1 / 62
700 likes | 959 Views
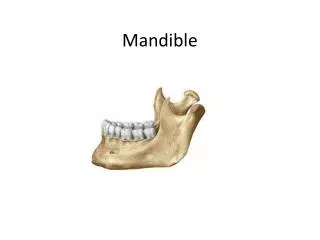
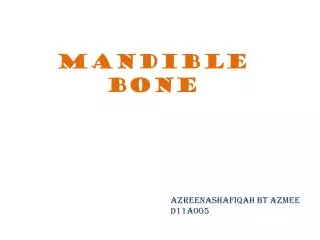
Mandible Fractures. Innervation. CNV3, the mandibular n., through the foramen ovale Inferior alveolar n. through the mandibular foramen Inferior dental plexus Mental n. through the mental foramen. Arterial Supply. Endosteal blood supply Inferior alveolar artery Mental artery

E N D
Innervation • CNV3, the mandibular n., through the foramen ovale • Inferior alveolar n. through the mandibular foramen • Inferior dental plexus • Mental n. through the mental foramen
Arterial Supply Endosteal blood supply • Inferior alveolar artery • Mental artery Periosteal blood supply (old age)
Musculature: Jaw Elevators • Masseter: Arises from zygoma and inserts into the angle and ramus • Temporalis: Arises from the infratemporal fossa and inserts onto the coronoid and ramus • Medial pterygoid: Arises from medial pterygoid plate and pyramidal process and inserts into lower mandible
Musculature: Jaw Depressors • Lateral pterygoid: lateral pterygoid plate to condylar neck and TMJ capsule • Mylohyoid: mylohyoid line to body of hyoid • Digastric: mastoid notch to the digastric fossa • Geniohyoid: inferior genial tubercle to anterior hyoid bone
Epidemiology • Mandible most common after nasal fractures • Mandible : Zygoma : Maxilla 6:2:1 • Ellis 4711 facial fractures, 45% with mandible fractures • Assault>MVA>Fall>Sports
Males > females; 3 to 1 • Most prevalent age range: 16-30 year old • Concomitant injuries are common • Must rule out spinal injuries • Dental injuries are commonly associated with other facial fractures
Epidemiology • Sites of weakness • Third molar (esp. impacted) • Socket of canine tooth • Condylar neck
Epidemiology • Boole et al ( 5196 fractures) • Young military men • Angle 35%, Symphysis 20%, Body 12%, Condylar 9%, Subcondylar 4%, Ramus 4%, Alveolar 3%, Coronoid 1% • 70% 1 fracture, 30% 2 fractures, .2% more than 2 • Facial lacerations 30%, other facial fracture 16%, C-spine 0.8%
Classifications of Fractures • Simple or closed fracture • Compound or open fracture • Comminuted fracture • Greenstick fracture • Pathologic fracture • Favorable vs Unfavorable fracture
Classifications of Fractures • . According to the severity of the injury • Simple fracture: In which the soft tissue, that may be damaged, but there is no open wound communicating the fracture fragment with the outside. • Compound fracture: In which there is an open wound with direct communication of the fragments with the out side.(all body # are compound because are open in PDL)
According to the type of fracture • Green stick fracture: There is incomplete discontinuity of the bone occurs in children. • Complex fracture: In which the fracture occurs in more than one bone. • Comminuted fracture: In which the bone is fractured into many fragments. • Pathological #
Unilateral fracture: Usually single, but occasional more than one fracture line may be present in one side. • Bilateral fracture: Usually occur from combination of direct and indirect force, e.g. angle and opposite condylar fracture. • Multiple fracture: Also occurs from the direct indirect force combination, e.g. symphyseal and bilateral condylar fracture(parade fracture)
According to the cause • Direct force: A direct blow to the mandible is the most common cause of mandibular fracture. • Indirect force: Fracture may occur from a blow applied at a distance from the fracture site, e.g. a blow to the symphysis may cause subcondylar fracture. • Excessive muscular contraction: This may cause fracture as with electric shock therapy, (Coronoid #)
Anatomic Region Classification • Condylar process • Coronoid • Ramus • Angle • Body • Symphysis or Parasymphysis • Alveolar process
According to the direction of the fracture line • The fracture line may be horizontal or vertical, each may be favorable or unfavorable.
In Angle area Masseter, Medial and Lateral Pterygoid, and Temporalis tend to draw fractures medial and superior • Medial Pterygoid is the stronger component • This is affected by the vertical or horizontal direction fracture line
Favorable vs. Unfavorable • Unfavorable Fractures where the muscles tend to draw fragments apart • Most angle fractures are horizontally unfavorable • Most parasymphyseal fractures are vertically unfavorable • Symphyseal # are favorable why?
Evaluation • Stabilization via ATLS protocol • Part of secondary survey • Blow to face favors parasymphyseal fracture and contralateral angle fracture • Fall to chin (bilateral condylar fractures)
Evaluation • Previous occlusion (Class I-III)(photos) • Psychiatric, seizure disorders • Previous facial trauma • Other injuries (c-spine, intra-abdominal, likely prolonged intubation)
Evaluation Common symptoms of mandibular fracture • Pain: Especially with motion, • Tenderness: Palpation over the fracture site reveals tenderness. • Disability: The patient is unable to open the mouth normally. • Swelling: Swelling early after injury is due to escape of blood at the fracture site.
Evaluation • Discoloration: The overlying tissue become red, bluish or purplish as a result of hemorrhage or haematoma formation. • Deformity: Displacement of the fractured fragment may be suggested by asymmetry of the face and deformity. • Abnormal mobility: The mandible will move in an abnormal way.
Evaluation • Crepitation: The patient may note a greeting, cracking or griding sound during movement as the fragments move in contact with each other. • Salivation: Pain and tenderness stimulate salivary secretion. Drooling of saliva from the mouth is increased by the inability to swallow the excessive saliva. • Bad odor: The patient may have offensive breath due to putrefaction of blood clots and mucous.
Extensive comminution or bilateral fracture of the symphyseal region may result in sever respiratory difficulties due to the posterior displacement of the fractured fragments
Physical Exam Signs Of Mandibular Fracture • Step defects \occlusion • Palpable step\ the inferior border • Tenderness to palpation • Malocclusion
Physical Exam • Trismus (35 mm or less) • Altered sensation of V3 • Crepitus • Unnatural mobility • Ecchymosis in floor of mouth (pathognomonic) • Mucosal lacerations
Physical Exam • Anesthesia of lower lip is “pathognomonic” of a fracture distal to the mandibular foramen (degree displacement) • The converse is not true: not all fractures distal to the mandibular foramen have mental n. anesthesia
Physical Exam • Dental Exam • Lost, fractured, or unstable teeth • Dental Health • Relation to fracture • Quantity
Inspection Sublingual ecchymosis Step defects, ridge discontinuity, malocclusion
Malocclusion • Step defects in the occlusion
Mucosal laceration • Step defects in the occlusion
PALPATION • “Step” Defect • Unnatural mobility • Crepitus • Bony segments • Subcutaneous emphysema • Mobility
Condylar Injuries • Contusion -Damage to the joint soft tissues leads to Synovial effusion, haemarthrosis -Symptoms are pain, limitation of mouth openning and tenderness over the joint - Accurate Dx need MRI - ttt soft diet, analgesics
Dislocation Displacement of the condyle from the glenoid foosa(see TMJ topics) • Fracture
Condylar Fracture Classification I According to the extend of the fracture line • A. Intracpsular fracture Fracture through the condylar head generally intracpsular. • B. Extracapsular fracture Fracture line extends through the neck of the condyle. • C. Subcondylar fracture; The fracture line runs from the sigmoid notch, downwards and posteriorly to the posterior border of the ramus
II. According to the position ofthe condylarfragment • A. Undisplaced fracture The fracture is complete but the fragments remain in their anatomical positions. • B. Displaced fracture The condylar head is displaced, medially and anteriorly but remains within the limits of the glenoid fossa • C. Dislocated fracture The condylar head is expelled from the fossa and out of the limits of the temporomandibular joint.
Physical Exam • Unilateral fractures of Condyle Decreased translational movement, and functional height of condyle ,lead to • Deviation of chin toward the fractured side, • open bite on the opposite side of fracture Bilateral fractures of condyle - Anterior open bite - Gaging of posterior teeth
Radiographic Exam • x-ray (image areas of concern with 2 films at 90o to one another: eg. peri-apicals & 90o occlusal ) • gaps • overlap • lost teeth • displaced teeth • foreign bodies • chest x-ray to locate missing pieces
Radiographic Exam Radiographs: • Panoral tomogram: the best single overall view of the mandible (if not available R\L oblique lateral é rotated PA) • PA mandible: to show medial or lateral displacement of fractured body\ angle. not suitable for TMJ • Reverse townes projection: for TMJ #
Radiographic Exam • intra-oral - Periapicals to show position& condition of teeth involved in # line - Occlosal views\ midline # with minimal displacement