Download
1 / 12
140 likes | 1.02k Views
Agonist vs Antagonist. Dr. Milton Leong. Gonadotrophin releasing hormone analogs. GnRH analogs: GnRH-like molecules 2 types of GnRHa: agonists and antagonists

E N D
Agonist vs Antagonist Dr. Milton Leong
Gonadotrophin releasing hormone analogs • GnRH analogs: GnRH-like molecules • 2 types of GnRHa: agonists and antagonists • Agonists initially enhance gonadotrophin released from the pituitary; but with continuing administration, cause down-regulation of the pituitary and reduced LH & FSH secretion • Antagonists bind onto GnRH receptors and completely suppress the pituitary hormone secretion within a few hours • Effects completely reversible after withdrawal
Agonists • GnRH agonists are used in common treatment protocols: • Long protocol – aims at complete pituitary suppression • Short & ultra-short protocols – utilize the “flare-up” effect • Usage in ART treatment is well established • Combining the use of agonists and gonadotropins in IVF cycles give high pregnancy rates after IVF and ET
Antagonists - 1 • GnRH antagonists can be administered as single dose or multi dose in either a fixed or a flexible protocol (Olivennes F et al, 2003; Mansour RT et al, 2003; Diedrich K et al, 2001) • Usage in ART treatment is relatively new • Advantages (Shapiro DB and Mitchell-Leef D, 2003): • shorter duration of injectable drug treatment • decreased gonadotropin requirement per cycle • improved patient convenience • lower overall treatment cost
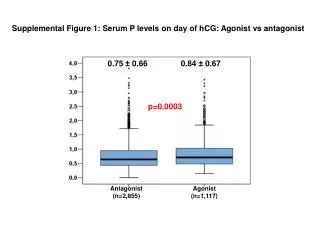
Antagonists - 2 • Bosch E et al (Fertil & Steril 2003; 80:1444-9) • Prospective observational study to determine the prevalence and the effect of premature luteinization in GnRH antagonist IVF-ET cycles • Antagonist was administered from stimulation day 6; serum P, E2, and LH were determined on the day of hCG administration • Premature luteinization is frequent during antagonist IVF-ET cycles and is associated with lower pregnancy and implantation rates • Progesterone elevations are not related to serum LH levels
Antagonists - 3 • Fanchin R et al (Fertil & Steril 2004; 81:1554-9) • Prospective longitudinal study to investigate whether premenstrual administration of antagonist coordinates early antral follicle sizes during the subsequent follicular phase • On cycle day 2 (control/day 2), early antral follicles were measured by ultrasound, serum FSH and ovarian hormones were also determined; on day 25, a single 3mg cetrorelix was administered. On the subsequent day 2 (antagonist/day 2), participants were re-evaluated as on control/day 2 • Follicular diameters and follicle-to-follicle size disparities were decreased • FSH, E2, and inhibin B were lower on antagonist/day 2 than on control/day 2
Antagonists - 4 • Acevedo B et al (Fertil & Steril 2004; 82:343-7) • Randomized controlled study in donor cycles receiving either antagonist alone or antagonist with rLH • A significant increase in MII oocyte (80% vs. 71%), fertilization rates (83% vs. 71%), G1 embryos (17% vs. 3%), and implantation rates (35% vs. 15%) in recipients whose embryos originated from donors receiving antagonist + rLH as compared to donors receiving antagonist alone • E2 levels, pregnancy/transfer and clinical pregnancies were lower (not significant) in donors treated with antagonist alone vs. those receiving the rLH-supplemented antagonist
Controlled Studies on Agonist vs Antagonist - 1 • Akman MA et al (Hum Reprod 2001, 16(5):868-70) • Prospective randomized trial on poor responders: group 1 – agonistic flare-up protocol group 2 – antagonistic multi-dose protocol • E2 levels on the day of hCG were lower in group 2 compared with group 1 • Clinical pregnancy and implantation rates did not show any significant difference • Limitation of this study: small sample size, with only 24 subjects in each group
Controlled Studies on Agonist vs Antagonist - 2 • Vlaisavljevic V et al (Reprod Biomed Online 2003, 7(3):301-8) • Prospective randomized study: group 1 – single dose long agonist (goserelin) protocol group 2 – single 3mg dose antagonist (cetrorelix) protocol, when the mean follicle diameter exceeded 12mm • The mean number of ampoules of FSH and the duration of stimulation were statistically significantly lower in group 2 than in group 1 (25.9 versus 34.5, and 9.6 versus 12.2 days, P < 0.01) • The mean number of oocytes retrieved, fertilization rates, blastulation rates and blastocyst transfer rates were similar in both groups • Clinical pregnancy and delivery rates per cycle were higher in group 1 (34.3 and 30.1%) than in group 2 (31.9 and 28.3%), but the differences were not statistically significant
Controlled Studies on Agonist vs Antagonist - 3 • Loutradis D. et al (Fertil & Steril 2004, 82(5):1446-8) • Prospective randomized study: group A – long protocol of agonist group B – modified multi-dose antagonist protocol, starting when the largest follicle had reached 14mm, with simultaneous augmentation of 75IU rFSH up to and including the day of hCG administration • No improved pregnancy and implantation rates
Meta-analysis on Agonist vs Antagonist - 1 • Ludwig M, Katalinic A, Diedrich K (Arch Gynecol Obstet 2001; 265(4):175-82) • A meta-analysis performed to evaluate whether there is a reduction in cases of severe OHSS and/or a reduction in pregnancy rates when using antagonists • Cetrorelix but not ganirelix will reduce the incidence of cases of OHSS • Cetrorelix but not ganirelix will result in the same pregnancy rates as the long agonist protocol
Meta-analysis on Agonist vs Antagonist - 2 • Al-Inany H and Aboulghar M (Hum Reprod 2002; 17:874-85) • A Cochrane review • 5 randomized trials were included, comparing fixed protocol of antagonist with long protocol of GnRH agonist • The clinical pregnancy rate was lower using antagonist • No significant difference in prevention of premature LH surge and prevention of severe OHSS