Download
1 / 12
120 likes | 151 Views
Trypanosoma brucie gambiense. Trisha Patel. “From the beginning of Arab and European influence in the hinterland of tropical Africa, trypanosomiasis of man and animals has curbed the realization of human ambitions and the mobilization of the continent’s vast resources.”

E N D
Trypanosoma brucie gambiense Trisha Patel “From the beginning of Arab and European influence in the hinterland of tropical Africa, trypanosomiasis of man and animals has curbed the realization of human ambitions and the mobilization of the continent’s vast resources.” --Herbert S. Gasser
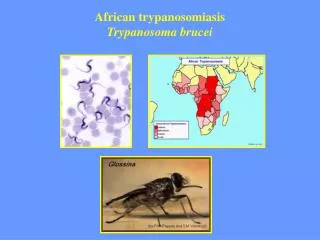
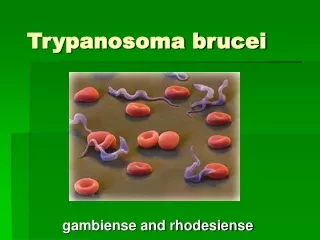
WEST AFRICAN SLEEPING SICKNESS • Found in western and central Africa • Transmitted human to human via tsetse fly vector • Slow onset of symptoms • Two stages: First stage- Before crossing the blood-brain barrier Second stage- After crossing the blood-brain barrier and entering the Central Nervous System
DISCOVERY The first documented case of Trypanasoma brucei was in 1902 by R.M. Forde. In The Journal of Tropical Medicine, Forde records his account of a 42 year-old European male colonialist who came to him in May 1901 in Gambia Colony. The patient complained about having a fever and malaise. Forde presumed the gentleman to have malaria and therefore gave him anti-malarial medication. After days the condition had remained the same. A blood sample from the patient was taken and it showed no malarial parasites. Later, Dutton, another physician from the Liverpool School of Tropical Medicine, identified the parasite within the patient’s blood as Trypanasoma brucei. Due to the location of the parasite within the patient, it is assume that the species was of T.b. gambiense.
TIMELINE • 14th Century: First described case in Mali • 1896- 1906: First major recorded endemic • 1902: R.M. Forde & Dutton identified one causative agent of the sleeping disease • 1903: Castellani working in Uganda observed the parasite in the cerebrospinal fluid of one of his patients • 1903: Sir David Bruce recognized Tsetse fly as vector • 1906: Ayres Kopke introduced Atoxyl, an arsenic compound, as a treatment • 1920: Second major recorded endemic (first noted by Jamrot, a colonel for the French army) • 1970- now: Third major recorded endemic • 1984: The World Health Organization (WHO) launched a program to control trypanosomiasis Sir David Bruce
MAJOR ENDEMICS • Three Major Endemics: • 1896 through 1906 (mostly in Uganda and the Congo Basin) • 1920 (several African countries) • -Contained due to screening of millions of people at risk • - The disease has practically disappeared from 1960-1965 • - Surveillance was relaxed causing a relapse • 1970-now • - With the help of the World Health Organization, national control programs, and nongovernmental organizations efforts to control the spread have been implemented
PREVELANCE Thirty-six countries in equatorial Africa could be affected, including 22 of the world's most underdeveloped countries. In the United States, 31 cases of trypanosomiasis have been reported; mostly Eastern Sleeping Sickness. In 1998, almost 40,000 cases were reported but about 300,000-500,000 went undiagnosed In the Congo, more people die from sleeping sickness than from AIDS. Fifty-five to 60 million people in equatorial Africa that are exposed to the risk of a bite from the tsetse fly. The number of cases have decreased. From 1998 to now, reported cases feel from 37,991 to 17,616. It costs about a thousand dollars to treat a victim of the parasite. Recently, in the Democratic Republic of Congo, Angola and Southern Sudan, prevalence has reached 50%. This is greater than those infected with HIV/AIDS in these areas.
SPREAD • Transmitted by Tsetse fly • War • A pregnant women pass it to her fetus (rare) • Through a blood transfusion (rare) • Homosexual males (very rare) • The migration of people
ENVIRONMENTAL CHANGES • Glossina papalis tsetse fly - lives near vegetation associated with drainage lines, rivers, and other permanent bodies of water • Removal of waterways are ineffective since: • They are also habitats for other insects and animals • They are a source of water for people • Vegetation around these areas need water • Sanitation of waterways will not effect the spread of the organism.
TREATMENT First stage treatments • Pentamidine: Discovered in around 1941 Highly effective Few side-effects; usually tolerable Second stage treatments • Melarsoprol: Discovered in 1949 Arsenic base Many side-effects including enchephalopathy, myocarditis, renal damage, peripheral neuropathy, etc. Fatal (3-10%) • Eflornithine: Also known as “the resurrection drug” Registered in 1990 Less toxic than melarsoprol Regime is strict and difficult to apply Costly
PREVENTION • Wear khaki or olive colored clothing • Wear thick clothing • Use insect repellant • Use bed netting when sleeping • Inspect vehicles for tsetse flies before entering • Do not ride in the back of jeeps, pickup trucks or other open vehicles • Avoid bushes (tsetse fly is less active during the hottest time of the day and rests in bushes—it will bite if disturbed) • Avoid thick shrubbery and trees by rivers and waterholes • Test blood during transfusions
SOURCES “African Trypanosomiasis.” African Sleeping Sickness. 22 May, 2001. 13 November, 2006. <http://www.stanford.edu/class/humbio103/ParaSites2001/trypanosomiasis/trypano.htm>. “Background to Trypanosoma brucei gambeinse genome project.” 13 November, 2006. <http://www.bio.bris.ac.uk/research/molpar/TBG.pdf#search='Trypanosoma%20brucei%20gambiense%20%20%20Discovery’>. “Behind the Frieze.” Sir David Bruce. London School of Hygiene and Tropical Medicine. 1 August, 2005. 16 November, 2006. <http://www.lshtm.ac.uk/library/archives/bruce.html>. “Google Image Search.” 19 November, 2006. <http://images.google.com/imghp?ie=UTF-8&oe=UTF-8&hl=en&tab=wi&q=>. “Reanalyzing the 1900–1920 Sleeping Sickness Epidemic in Uganda.” Center of Disease Control. 12 April, 2004. 16 November, 2006. <http://www.cdc.gov/ncidod/EID/vol10no4/02-0626.htm>. “Sleeping Sickness.” Wikimedia Foundation, Inc. 15 November, 2006. 16 November, 2006. <http://en.wikipedia.org/wiki/Sleeping_sickness#Treatment>. “Trypanosomiasis.” Microbiology @ Leicester. 19 October, 2004. 13 November, 2006. <http://www-micro.msb.le.ac.uk/224/Trypano.html>. “Trypanosomiasis/Sleeping Sickness.” Medindia Health Network Pvt Ltd. 13 November, 2006. 13 November, 2006. <http://www.medindia.net/patients/patientinfo/trypanosomiasis_Clinical.htm>. Watson, Debra. “War, famine and now pestilence.” Sleeping sickness ravages Central Africa. International Committee of the Fourth International. 5 September, 1998. 19 November, 2006. <http://www.wsws.org/news/1998/sep1998/slep-s05.shtml>.