Download
1 / 70
700 likes | 879 Views
"Bioterrorism Preparedness: Smallpox Contingency Planning". Dr Bonnie Henry Associate Medical Officer of Health, Emergency Services Unit, Toronto Public Health. Public Health Role. Health effects of emergencies recently highlighted MOH part of City EOC

E N D
"Bioterrorism Preparedness: Smallpox Contingency Planning" Dr Bonnie Henry Associate Medical Officer of Health, Emergency Services Unit, Toronto Public Health
Public Health Role • Health effects of emergencies recently highlighted • MOH part of City EOC • Mandated lead role in events involving biologic agents
Public Health Role • Early Detection • Mass Patient Care • Mass Immunization/Prophylaxis • Epidemiologic investigation • Command and Control
Public Health Role • Mass Fatality Management • Evacuations/sheltering • Environmental Surety • Community Recovery
Toronto Public Health Incident Management System Chair, Board of Health Medical Officer of Health Divisional Management Team Public Health Incident Manager Public Information Liaison Operations Planning Logistics Administration Claims/ Compensation Mass Vaccination/Post Exposure Prophylaxis Situation Assessment Facilities Staffing & Resource Needs Human Resources Hotline Operation Costing Reception Centre/Mass Care Procurement Resource Deployment Communications Equipment Miscellaneous Supplies Case Management/Contact Tracing Documentation Environmental Inspection/ Sampling Demobilization & Recovery Nutrition/staff accommodation Epidemiological Investigations Recovery
Bioterrorism is the intentional use of microorganisms (bacteria, viruses, and fungi) or toxins to produce death or disease in humans, animals or plants. Electron micrograph of anthrax bacteria Electron micrograph of ebola virus
Category A • “Biologic Threat Agents” • Can be easily disseminated or transmitted person-to-person; • Cause high mortality, w/potential for major public health impact; • Might cause public panic and social disruption; and • Require special action for public health preparedness.
Biological Agents of Highest Concern Category A • Smallpox – variola major • Anthrax – Bacillus anthracis • Plague – Yersinia pestis • Botulism – Clostridium botulinum toxin • Tularemia – Francisella tularensis • Viral hemorrhagic fevers – arenaviruses, filoviruses (Ebola, Marburg, Lassa, Junin)
Moderately easy to disseminate Cause moderate morbidity and low mortality Require specific enhancements of diagnostic capacity and enhanced disease surveillance Coxiella burnetti (Q fever) Brucella Burkholderia mallei (glanders) Alphaviruses (Venezuelan encephalomyelitis and Eastern and Western equine) Rickettsia prowazekii Toxins (Ricin, Staph enterotoxin B) Chlamydia psittaci Food safety threats (e.g.Salmonella, Shigella. E. coli O157:H7) Water safety threats (Vibrio cholerae, Cryptosporidium parvum) Category B: Second Highest Priority
Pathogens that could be engineered for mass destruction because of availability, ease of production and dissemination and potential for high morbidity and mortality and major health impact Nipah virus Hantavirus Tickborne hemorrhagic fever viruses Tickborne encephalitis viruses Yellow fever MDR TB Category C: Third Highest Priority
Characteristics of Bioterrorist Agents • Mainly inhaled - may be ingested or absorbed • Particles may remain suspended for hours • May be released silently with no immediate effect • Person-to-person spread happens for some agents • Long incubation periods mean "first responders” may be primary health care providers • Agents may be lethal or incapacitating • Vaccines & antitoxins exist for some agents
Recent Examples of Bioterrorism 1984: Salad bars contaminated with Salmonella to influence local election in Oregon / 751 people affected (8 salad bars) 1995: Sarin nerve gas release by Aum Shinrikyo in Tokyo subway / At least 9 failed attempts to use biological weapons 1996: Pastries contaminated with Shigella by disgruntled lab worker in Dallas
Recent Examples of Bioterrorism Former Soviet Union’s extensive biological weapons program thought to have found their way to other nations Iraq acknowledged producing and weaponizing anthrax and botulinum toxin Currently, at least 17 nations believed to have biological weapons programs
Anthrax: Soviet incident An accident at a Soviet military compound in Sverdlovsk (microbiology facility) in 1979 resulted in an estimated 66 deaths downwind.
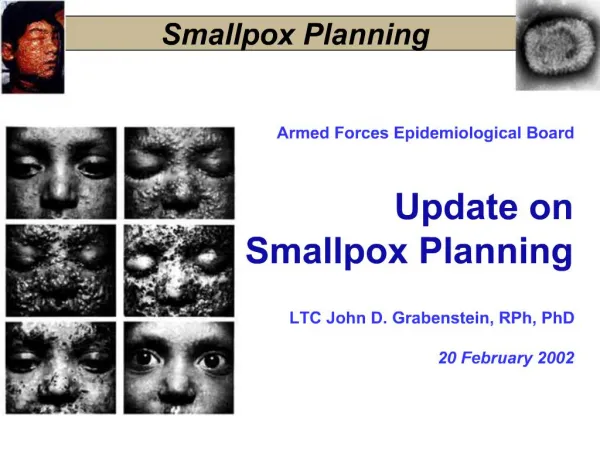
Smallpox • Variola virus • Declared eradicated by WHO in 1980 • Civilian vaccination stopped 1972, healthcare workers stopped in 1977 and CF stopped 1988 • Known stockpiles remain in CDC and Institute for Viral Preparations, Moscow • Virus spread by aerosol • Incubation period: average 12 days (7-19 days)
Last Case, Variola major Rahmina Banu, 2001 Rahmina, 1975
Smallpox • Clinical symptoms: abrupt onset of malaise, fever, rigors, headache, emesis, backache, delirium (15%) • Onset of rash 2-3 days later on face, hands, forearms, and legs, then spreading centrally • Lesions progress from macules to papules to pustular vesicles • Lesions typically in same stage of development • Patients highly infectious during initial respiratory phase and until all eschars are off • Mortality in unvaccinated about 30%
SMALLPOX RASH EVOLUTION Day 1 Day 2 Day 3
SMALLPOX RASH EVOLUTION Day 4 Day 5 Day 7
SMALLPOX RASH EVOLUTION Days 8-9 Days 10-14 Day 20
Variola Varicella Centrifugal Centripetal Lesions all at the same stage Lesions in various stages Slow evolution Rapid evolution Deep lesions: circular and regular Scarring: severe Superficial lesions: oval or irregular Scaring: Mild Smallpox Characteristics differentiating the rashes of Smallpox and Varicella
Smallpox • Vaccination • Within 3 days will likely prevent disease • Within 5 days is life-saving (ameleorates) • Canada has about 320,000 doses • ?long term immunity • Cell culture and oral vaccine in research • Research on antivirals also ongoing (particularly Cidofovir)
Type Proportion of cases (%) Case fatality rate (%) Variola major 90 30 Variola minor 2* <1 Hemorrhagic <3 100 Flat/malignant 7 97 TYPES OF SMALLPOX * 25% of vaccinated cases present as variola minor
DIFFERENTIAL DIAGNOSIS: VESICULO – PUSTULARRASHES • CHICKEN POX • ERYTHEMA MULTIFORME - BULLOUS • COWPOX • MONKEY POX • HERPES ZOSTER (Shingles) - DISSEMINATED • DRUG ERUPTIONS • HAND FOOT AND MOUTH DISEASE • ACNE • IMPETIGO • INSECT BITES
“Moderately” contagious Virus not robust No natural reservoir Able to vaccinate Able to control Improved medical care Better pop’n health 30% mortality Misdiagnosis Long incubation Low level of “Immunity” Pop’n mobility Immuno-compromised Mass panic, hysteria Today’s Perspective in Canada:Pros vs Cons
Canada’s ‘search and contain’ strategy highlights: Early detection, immediate notification Immediate isolation of cases Immediate deployment of smallpox responders Immediately vaccinate all those directly exposed, all known direct contacts, all local personnel… Intensive contact tracing Rapid set up of isolation facilities Rapid set-up of local Smallpox assessment centres Assumption: In the absence of smallpox anywhere in Canada A risk of disease and death from a vaccine, no matter how small, may be unacceptable Especially when pre-attack vaccination is considered National Smallpox Contingency Plan (v.4)
Political Divisions • Canada’s search and contain strategy consists primarily of public health measures, which fall under provincial/territorial jurisdiction • Federal role: • Immediate mobilization of vaccine • Deployment of ‘federalized’ smallpox response teams (SERF) • Provision of supplies • 24-hour support line to the public, professional and other governments • International notification and consultation
“WHO’s success with isolation” WHO’s experience in India : • 1960 – 1973 Smallpox transmission continued during this time under a mass vaccination strategy. • In 1973, a search and containment strategy was introduced, stressing isolation of cases. • Smallpox was then eliminated in just two years, in 1975. We will come back to this….
VACCINE CONTRAINDICATIONS • History or presence of eczema • Other acute , chronic or exfoliative skin condition • Immunosuppression ( HIV, AIDS, cancer, immunodeficiency disorders, chemotherapy, radiotherapy, organ transplant, high dose corticosteroids • Pregnancy • History of anaphylaxis to a vaccine component
Complication Primary vaccination* Revaccination* Inadvertent inoculation 529 42 Generalized vaccinia 242 9 Erythema multiforme 165 10 Eczema vaccinatum 39 3 Postvaccinial encephalitis 12 2 Progressive vaccinia 2 3 Other 266 39 VACCINATION: RATES OF COMPLICATIONS * No. of events per million vaccinations Source: NEJM 346 (17) April 2002; Data from 1968 survey of 10 States
Consider Recent Smallpox Response Models • Kaplan et al. (Proc Natl Acad Sci USA) • Halloran et al. (Science) • [Mention: • Epstein et al. (Brookings Working Paper) • Bozzette et al. (N Eng J Med)]
Technical Discussions Highlight Different Modeling Approaches • Kaplan et al. – free mixing; explicit logistics • Halloran et al. – “structured stochastic simulation” • [Epstein et al. – agent-based • Bozzette et al. – simulation with assumed response efficacy from historical data]
Other Factors Matter More • Scale of model • Kaplan et al. consider population of 10 million • Halloran et al. look at “community “ of 2,000 • [Epstein et al. consider “county” of 800 • Bozzette et al. – no role for population in model]
Other Factors Matter More • Rate of vaccination and logistics • Traced (ring, targeted) vaccination proceeds with the pace of the epidemic – need to see symptomatic cases to trigger vaccination • Mass vaccination proceeds at a pace limited only by available resources • number of vaccinators • time required to vaccinate
Important To See If Models Have Different Policy Implications • To do so, need to control for inputs as much as possible to see if different assumptions on model structure lead to different results
Kaplan et al. (PNAS) • Focus on a large city (10,000,000) • Construct “traced vaccination” (TV) model • Contrast with “mass vaccination” (MV) • Consider TV/MV switch if TV fails to control outbreak after 2 generations of cases • Consider pre-attack vaccination
Kaplan et al. (PNAS) • Disease transmission/progression: 4 disease stages (includes infected but vaccine sensitive), free mixing in population (“worst case”), imperfect vaccination and (low) vaccine-related mortality • Response logistics: consistent tracing with disease transmission/progression linked to index case (“race to trace”), TV queues (finite TV capacity), MV rate higher than TV rate, quarantine capacity requirements • State transitions governed by both disease transmission/progression and response logistics; epidemic and response are on the same time scale!
TV or MV: 50% Tracing Accuracy • MV is optimal (fewer deaths) for any R0 > 1.3
TV or MV: 100% Tracing Accuracy • Still favor MV for any R0 > 2 • If initial attack > 20, favor MV for R0 > 1.3 (same as 50% tracing accuracy)
TV or MV: Asymmetries • Consequences of choosing the wrong policy are not symmetric! • If TV is optimal, choosing MV would lead to few incremental deaths • If MV is optimal, choosing TV could lead to a disaster with many incremental deaths • Would therefore suggest choosing TV only if extremely confident (i.e. highly certain) that initial attack size and R0fall on the TV-favorable side of the tradeoff curve
The Post-Attack Decision Expected Deaths Big Attack d (TV | Big) b Traced Vaccination 1- b d (TV | Small) Small Attack Big Attack d (MV | Big) b Mass Vaccination 1- b d (MV | Small) Small Attack
The Post-Attack Decision: Example • Suppose attack/response yields deaths as: • Choose MV if b > 7.4 x 10-5
Switching Helps, But Delay is Costly • In base case, switching from TV to MV after two generations of cases (28 days) results in 15,570 cases and 4,680 deaths • Cost of delay is high – 4,120 incremental deaths compared to MV • Given option to switch, still would only start with TV if extremely confident that both R0 and initial attack size are small
Pre-Attack Vaccination • Reduces degree of susceptibility in the population • Effect is to reduce R0 and initial attack size • Pre-attack vaccination makes post-attack TV more attractive as a result