Download
1 / 47
470 likes | 522 Views
Martini’s Visual Anatomy and Physiology First Edition Martini w Ober. Chapter 20 - Respiratory System Lectures 12 & 13. Midterm Grades. Your midterm grades (due March 28) will be calculated as follows:

E N D
Martini’s Visual Anatomy and Physiology First Edition Martini w Ober Chapter 20 - Respiratory System Lectures 12 & 13
Midterm Grades Your midterm grades (due March 28) will be calculated as follows: Lec 1 Exam 100 pointsLec 2 Exam 100 pointsLab 1 Exam 100 pointsLaboratory Grade 25-35 points (5-7 labs so far)Extra Credit 4 points Total points possible so far...329-339 points Your grade… (Ex., Total points you have / 330) * 100 Note:Nogrades will be dropped for calculation of midterm grade.
Mid-term Checkup Based on the three (3) grades you have received so far, you should do a mid-term checkup. To find your average so far total the following points: Lec Exam 1 + Lec Exam 2 + Lab Exam 1 + Lab points (6 labs) Example: (83 + 67 + 90 + 26) 330 = 0.80 (80%) Dropping the low grade: (83 + 90 + 26) 230 = 0.86 (86%) To figure out what you need to AVERAGE for the next lecture and/or lab exam and the final COMBINED to get a particular grade: Average grade needed on remaining exams* Points desired (see syllabus) – Total points so far = 350 (if no grade dropped) or 450 (if low grade dropped) *This formula assumes you will have 50 pts for lab and 6 XC pts at the end of the course
Points and Grades (from Syllabus) - Revised Example 1: To get a grade of B for the course, using the example grades on previous slide, and not dropping lowest grade (50), and assuming 50 pts for lab and 6 XC points: 574 – (83 + 67 + 90 + 50 + 6) = x; x = 0.79 (79%) Average on upcoming exams 350 Example 2: To get a grade of B for the course, using the example grades on previous slide, and dropping lowest grade (67), and assuming 50 pts for lab and 4 XC points: 574 – (83 + 90 + 50 + 6) = x; x = 0.76 (76%) Average on upcoming exams 450
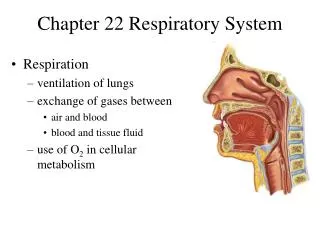
Lecture Overview • Lectures 12 & 13 • The breathing mechanism (ventilation) • Respiratory volumes and capacities • Nonrespiratory air movements • Alveolar gas exchange • Transport of O2 and CO2 in the blood • Control of breathing • Factors affecting breathing
Gases and Pressure • Our atmosphere is composed of several gases and exerts pressure • 78% N2, 21% O2, 0.4% H2O, 0.04% CO2 • 760 mm Hg, 1 ATM, 29.92” Hg, 15 lbs/in2,1034 cm H2O • Each gas within the atmosphere exerts a pressure of its own (partial) pressure, according to its concentration in the mixture (Dalton’s Law) • Example: Atmosphere is 21% O2, so O2 exerts a partial pressure of 760 mm Hg. x .21 = 160 mm Hg. • Partial pressure of O2 is designated as PO2
Air Movements If Volume increases, pressure decreases and vice versa Stated mathematically: P 1/V (Boyle’s Law) • Moving the plunger of a syringe causes air to move in or out • Air movements in and out of the lungs occur in much the same way Figure from: Saladin, Anatomy & Physiology, McGraw Hill, 2007
Lungs at Rest When lungs are at rest, the pressure on the inside of the lungs is equal to the pressure on the outside of the thorax Figure from: Hole’s Human A&P, 12th edition, 2010 Think of pressure differences as difference in the “concentration” of gas molecules and use the rules of diffusion. Higher pressure means higher concentration (ignoring temperature difference)
Normal Inspiration An active process • Intra-alveolar (intrapulmonary) pressure decreases to about 758 mm Hg as the thoracic cavity enlarges • Atmospheric pressure (now higher than that in lungs) forces air into the airways • Compliance – ease with which lungs can expand Figure from: Hole’s Human A&P, 12th edition, 2010 Phrenic nerves of the cervical plexus stimulatediphragm to contract and move downward and external (inspiratory) intercostal muscles contract, expanding the thoracic cavity and reducing intrapulmonary pressure. Attachment of parietal pleura to thoracic wall pulls visceral pleura, and lungs follow.
Maximal (Forced) Inspiration Thorax during normal inspiration • Thorax during maximal inspiration • aided bycontraction ofsternocleidomastoid and pectoralis minor muscles Compliance decreases as lung volume increases Costal (shallow) breathing vs. diaphragmatic (deep) breathing Figure from: Hole’s Human A&P, 12th edition, 2010
Normal Expiration • due to elastic recoil of the lung tissues and abdominal organs • a PASSIVE process (no muscle contractions involved) Normal expiration is caused by - elastic recoil of the lungs (elastic rebound) and abdominal organs - surface tension between walls of alveoli (what keeps them from collapsing completely?) Figure from: Hole’s Human A&P, 12th edition, 2010
Maximal (Forced) Expiration Figure from: Hole’s Human A&P, 12th edition, 2010 • contraction of abdominal wall muscles • contraction of posterior (expiratory) internal intercostal muscles • An active, NOT passive, process
Terms Describing Respiratory Rate • Eupnea – quiet (resting) breathing • Apnea – suspension of breathing • Hyperpnea – forced/deep breathing • Dyspnea – difficult/labored breathing • Tachypnea – rapid breathing • Bradypnea – slow breathing Know these
Nonrespiratory Air Movements • coughing – sends blast of air through glottis and clears upper respiratory tract • sneezing – forcefully expels air through the nose and mouth • laughing – deep breath released in a series of short convulsive expirations • crying – physiologically same as laughing • hiccupping – spasmodic contraction of diaphragm against closed glottis • yawning – deep inspiration through open mouth • valsalva maneuver – expiration against a closed glottis
Alveoli and Respiratory Membrane • consists of the walls of the alveolus and the capillary, and the basement membrane between them Figure from: Hole’s Human A&P, 12th edition, 2010 Mechanisms that prevent alveoli from filling with fluid: 1) cells of alveolar wall are tightly joined together 2) the relatively high osmotic pressure of the interstitial fluid draws water out of them 3) there is low pressure in the pulmonary circuit Surfactant resists the tendency of alveoli to collapse on themselves.
Just a Quick Review! • Atmosphere is composed of several gases, each exerting its own partial pressure, PO2 • P 1/V (Boyle’s Law) • Inspiration • Normal • Forced or maximal • Expiration • Normal • Forced or maximal • The respiratory membrane for gas exchange
Blood Flow Through Alveoli Mechanisms that prevent alveoli from filling with fluid: • cells of alveolar wall are tightly joined together • the relatively high osmotic pressure of the interstitial fluid draws water out of them • there is low pressure in the pulmonary circuit Low pressure circuit Figure from: Hole’s Human A&P, 12th edition, 2010
Diffusion Across Respiratory Membrane Figure from: Hole’s Human A&P, 12th edition, 2010
Diffusion Through Respiratory Membrane The driving for the exchange of gases between alveolar air and capillary bloodis the difference in partial pressure between the gases. Figure from: Hole’s Human A&P, 12th edition, 2010 At a given temperature, the amount of a particular gas in solution is directly proportional to its partial pressure outside the solution (Henry’s Law)
Composition of Inspired and Alveolar Air From: Saladin, Anatomy & Physiology, McGraw Hill, 2007
Factors Affecting O2 and CO2 Transport • O2 and CO2 have limited solubility in plasma • This problem is solved by RBCs • Bind O2 to hemoglobin • Use CO2 to make soluble compounds • Reactions in RBCs are • Temporary • Completely reversible
Oxygen Transport • Most oxygen binds to hemoglobin to formoxyhemoglobin (HbO2) • Oxyhemoglobin releases oxygen in the regions of body cells • Much oxygen is still bound to hemoglobin in the venous blood Figure from: Hole’s Human A&P, 12th edition, 2010 Tissues Lungs But what special properties of the Hb molecule allow it to reversibly bind O2?
Review of Hemoglobin’s Structure Figure From: Martini, Anatomy & Physiology, Prentice Hall, 2001
The O2-Hb Dissociation Curve Figure from: Hole’s Human A&P, 12th edition, 2010 Recall that Hb can bind up to 4 molecules of O2 = 100% saturation At 75% saturation, Hb binds 3 molecules of O2 on average Sigmoidal (S) shape of curve indicates that the binding of one O2 makes it easier to bind the next O2 This curve tells us what the percent saturation of Hb will be at various partial pressures of O2
Oxygen Release • Amount ofoxygen released from oxyhemoglobinincreases as • partial pressure of carbon dioxide increases • the blood pH decreases and [H+] increases (Bohr Effect; shown below) • blood temperature increases (not shown) • concentration of 2,3 bisphosphoglycerate (BPG) increases (not shown) Figure from: Hole’s Human A&P, 12th edition, 2010
Carbon Dioxide Transport in Tissues • dissolved in plasma (7%) • combined with hemoglobin as carbaminohemoglobin(15-25%) • in the form of bicarbonate ions (68-78%) CO2 + H2O ↔ H2CO3 H2CO3 ↔ H+ + HCO3- Figure from: Hole’s Human A&P, 12th edition, 2010 CO2 exchange in TISSUES
Chloride Shift • bicarbonate ions diffuse out RBCs • chloride ions from plasma diffuse into RBCs • electrical balance is maintained Figure from: Hole’s Human A&P, 12th edition, 2010
Carbon Dioxide Transport in Lungs Figure from: Hole’s Human A&P, 12th edition, 2010 CO2 exchange in LUNGS
Control of Respiration • Homeostatic mechanisms intervene so that cellular gas exchange needs are met • Control occurs at two levels • Localregulation • Lung perfusion (blood flow; ~5.5 L/min) • Alveolar ventilation (~4.2 L/min) • Ventilation/perfusion coupling (matching) • Respiratorycenter of the brain
Local Control of Respiration • Local Control regulates… • Efficiency of O2 pickup in the lungs • Lung perfusion (blood flow) • Alveolar capillaries constrict when local PO2 is low • Tends to shunt blood to lobules with high PO2 • Alveolar ventilation (air flow) • High PCO2 (hypercapnia) causes bronchodilation • Low PCO2 (hypocapnia) causes bronchoconstriction • Directs airflow to lobules with higher PCO2 • Rate of O2 delivery in each tissue • Changes in partial pressures • Local vasodilation in peripheral tissues
Factors Affecting Resistance to Airflow • Diameter of bronchioles • Bronchodilation (epinephrine, sympathetic stimulation) • Bronchoconstriction (parasympathetic stimulation, histamine, cold air, chemical irritants) • Pulmonary compliance • Surface tension of alveoli and distal bronchioles.
Neural Control of Respiration Figure from: Hole’s Human A&P, 12th edition, 2010 Neural control of respiration has an autonomic as well as a voluntary component
Respiratory Center – Autonomic Control Figure from: Hole’s Human A&P, 12th edition, 2010 - 2 sec / 3 sec - + Apneustic area Respiratory centers can be facilitated (caffeine, amphetamines) or depressed (opioids, barbiturates)
Factors Affecting Breathing Central chemoreceptors Respond to PCO2 and pH of the CSF Effect is actually due to [H+] as follows: CO2 + H2O ↔ H2CO3 H2CO3↔ H+ + HCO3- Bicarbonate Carbonic acid Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001
Factors Affecting Breathing Both central and peripheral chemoreceptors are subject to adaptation Decreased blood PO2 or pH (or increased CO2) stimulates peripheral chemoreceptors in the carotid and aortic bodies Stimulation leads to anincrease in the rate and depth of respiration Figure from: Hole’s Human A&P, 12th edition, 2010 CO2 is the most powerful respiratory stimulant
Control of Respiration • Control of respiration is accomplished by: 1) Local regulation 2) Nervous system regulation • Local regulation • alveolar ventilation (O2), Blood flow to alveoli • alveolar ventilation (O2), Blood flow to alveoli • alveolar CO2, bronchodilation • alveolar CO2, bronchoconstriction
Control of Respiration • Nervous System Control • Normal rhythmic breathing -> DRG in medulla • Forced breathing -> VRG in medulla • Changes in breathing • CO2 is most powerful respiratory stimulant • Recall: H2O + CO2↔ H2CO3 ↔ H+ + HCO3- • Peripheral chemoreceptors (aortic/carotid bodies) • PCO2, pH , PO2 stimulate breathing • Central chemoreceptors (medulla) • PCO2, pH stimulate breathing
Breathing Reflexes • Protective Reflexes • Sneezing - Triggered by an irritation of the nasal cavity • Coughing – Triggered by an irritation of the larynx, trachea, or bronchi • Both sneezing and coughing involve • A period of apnea • Forceful expulsion of air from lungs opening the glottis (up to 100 mph or more!!) • Laryngeal spasms – chemical irritants, foreign objects, or fluids into the area around glottis • Temporarily closes the airway • Some stimuli, e.g., toxic gas, can close the glottis so powerfully that it doesn’t open again!
Clinical Application The Effects of Cigarette Smoking on the Respiratory System Figure from: Hole’s Human A&P, 12th edition, 2010 • cilia disappear • excess mucus produced • lung congestion increases lung infections • lining of bronchioles thicken • bronchioles lose elasticity • emphysema fifteen times more common • lung cancer more common • much damage repaired when smoking stops
Clinical Application Figure from: Martini, “Fundamentals of Anatomy & Physiology”, Pearson Education, 2006
Review • The atmosphere is composed of a mixture of gases • Each gas exerts a partial pressure (Pg) • Sum of all partial pressures = atmospheric pressure (14.7 lbs/in2,760 mm Hg., …) • Gases move from a higher concentration (pressure) to a lower concentration (pressure) • Function of the diaphragm is to create a lower intrpulmonary pressure so that atmospheric gases flow into the lungs
Review • Normal inspiration • An active process • Phrenic nerve and diaphragm • External (inspiratory) intercostal muscles • Role of the lung pleura • Normal expiration • A PASSIVE process • Due to elasticity of lung/abdominal organs and alveolar surface tension • Forced inspiration • Forced expiration
Review • Oxygen travels in the blood bound to Hb • Four O2 molecules can be bound to 1 Hb • O2 bound to Hb - oxyhemoglobin • Uptake and release of O2 is dependent upon PO2 in alveoli and tissues • Several factors can increase the release of O2 from Hb • Increased PCO2 • Increased [H+] (decreased pH) • Increased temperature of blood
Review • Carbon dioxide can travel in several ways • Dissolved in plasma (7%) • As carbaminohemoglobin (15-25%) • As HCO3- ion (70%) • Recall: H2O + CO2↔ H2CO3 ↔ H+ + HCO3- • Carbonic anhydrase in RBCs accelerates interconversion between CO2 and HCO3- • H+ combines with or dissociates from Hb • HCO3- diffuses into plasma or into RBCs • Cl- diffuses into RBC (chloride shift) as HCO3- exits • Diffusion of CO2 is related to PCO2 in alveoli and tissues
Review • The respiratory membrane • Simple squamous epithelium of the alveoli and capillaries • Basement membrane between them • Terms used to describe breathing (know these)
Control of Respiration • Control of respiration is accomplished by: 1) Local regulation 2) Nervous system regulation • Local regulation • alveolar ventilation (O2), Blood flow to alveoli • alveolar ventilation (O2), Blood flow to alveoli • alveolar CO2, bronchodilation • alveolar CO2, bronchoconstriction
Control of Respiration • Nervous System Control • Normal rhythmic breathing -> DRG in medulla • Forced breathing -> VRG in medulla • Changes in breathing • CO2 is most powerful respiratory stimulant • Recall: H2O + CO2↔ H2CO3 ↔ H+ + HCO3- • Peripheral chemoreceptors (aortic/carotid bodies) • PCO2, pH , PO2 stimulate breathing • Central chemoreceptors (medulla) • PCO2, pH stimulate breathing