Download

1 / 133
1.5k likes | 2.29k Views
Transthoracic Echo. in the I.C.U and emergency department . Case presentation & literature review. Case presentation . Two cases. Dr. Saad Subahi Consultant cardiologist at ALRIBAT university hospital . Case (1) .

E N D
Transthoracic Echo. in the I.C.U and emergency department Case presentation & literature review
Case presentation Two cases
Dr. SaadSubahi • Consultant cardiologist at ALRIBAT university hospital
46 old male admitted electively to hospital on 12/05/2010 for lamincectomy
MRI showed disc prolapse at L4&5 • No significant P.H
Next morning (13/05/2010) he had inter laminar discetomy, done under G.A. • Uneventful course
2nd post-operative day, at 10:30 a.m (Friday) he was seen by the neurosurgeon • Patient was comfortable, apart from minimal backache • Vitals were stable • He was advised to mobilize out of bed
Immediately after mobilization patient developed sudden SOB; taken back to bed, noticed to be sweaty with cold extremities .
Soon, prior to any intervention, respiratory and subsequently, cardiac arrest ensued
Advanced cardiac life support was immediately implemented. • After resumption of spontaneous circulation he was transferred to ICU
Before connecting him to M.V. he had second arrest; CPR (for 3 minutes) -----> Resumption of spontaneous circulation
Given 2 liters of N/S because of B.P of 75/45, followed by dopamine infusion, titrated up to 20mcg/kg/min
He was connected to M.V. at 11:0 a.m • I attended the patient at 11.30 am
Vital signs : pulse 145/min; B.P : 88/52; oxygen sat 99% • There was prominent jugular venous distention.
The lungs were clear on auscultation, with normal breath sounds
12-lead ECG showed sinus tachycardia, “S 1Q 3T 3” pattern & RBBB • Chest x-ray : normal • CBC, Urea & electrolytes were normal
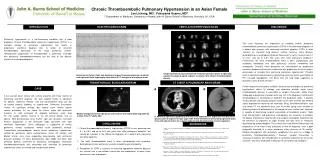
A presumptive diagnosis of massive pulmonary embolism was made .
Dr Saad • ECHO • Daignosis • Discussed with the neurosurgeon and started on streptokinase 1.5 million units, over one hour . • Events during streptokinase infusion . • Hypotension & bradycardia • Severe biventricular dysfunction ------- adrenaline infusion • Improvement in biventricular function, pulse rate & blood pressure • D/C of adrenaline infusion • Maintenance of normal B.P • Recovery of RT ventricular function
Diagnosis: Massive PE-induced cardiac arrest + right heart thrombi-in-transit
At 10:0 am : • Improvement in BP & O2 saturation, & he was obeying commands
Shifted to spontaneous mode : TV > 300ml, rate 25-28/min & oxygen saturation 100% on FIO2 0.40
Accordingly he was extubated and connected to oxygen by simple mask (50%)
ABG 30 min post extubation : • PH : 7.35 • PCO2 : 37 mmHg • PO2 : 163 mmHg • O2 sat : 99% • HCO3 : 22 mmol/L • BE : -3 mmol/L
Time from clinical suspicion to thrombolytic therapy : one hour
33 years female presented to the emergency room with 2 hours history of sudden shortness of breath • 3/08/2011 at 10.0 am
One week prior to presentation she had bilateral fracture of the tibial shaft (RTA), treated conservatively at home (long leg casting) . • Was completely confined to bed .
On presentation to A&E • Tachypnic : 40/min • Pulse : 140/min. • B/P : 70/35 • Confused & restless • Normal 1+11 heart sounds • Chest : normal auscultation
ECG : sinus tachycaria , inverted T- in V1-3 • ABG (NRM) : PH : 7.29 PCO2 : 31 mmHg PO2 : 66 mmHg HC03 : 16 mmol/l
ECHO : done by Dr Saad, within 15 min from time of presentation . • 1 liter of N/S, followed by dopamine infusion
Started immediately on IV streptokinase 1.5 million units over one hour .
ARRESTED : CPR was carried and streptokinase infusion was continued during CPR • She was intubated and CPR continued for 12 min ------ > ROSC
Transferred to ICU on dopamine infusion • Connected to the ventilator
Improvement of oxygenation, but continued to require inotropics
On the same day she had 2nd arrest at 9:30 pm . • CPR for five minutes ------> ROSC
Hospital course • AKI required peritoneal dialysis • Acute peritonitis • Recovered with a polyuric phase, during which she developed massive hematuria .
On day 5 : massive upper GIT bleeding required blood transfusion. • On day 7 : blocked ETT.
Day 11 on mechanical ventilation, she satisfied all extubation criteria . • She was extubated and connected to oxygen by simple mask .
After 29 days in ICU she was transferred to the ward, fully conscious and oriented with normal renal function; and discharged home 5 days later .
Time from clinical suspicion to thrombolytic therapy : 20 min.