Download
1 / 1
10 likes | 95 Views
No. 109. Contemporary use of partial Nephrectomy in Victoria for small r enal m asses – Good value for nephrons?. Anthony D. Ta 1,2 , Victoria White 3 , Graham G. Giles 2,3 , Ian D. Davis 4 , Margaret K. Dimech 3 , Jeremy Millar 5 , Damien M. Bolton 1,2 , and the IMPROVE Study Team 3

E N D
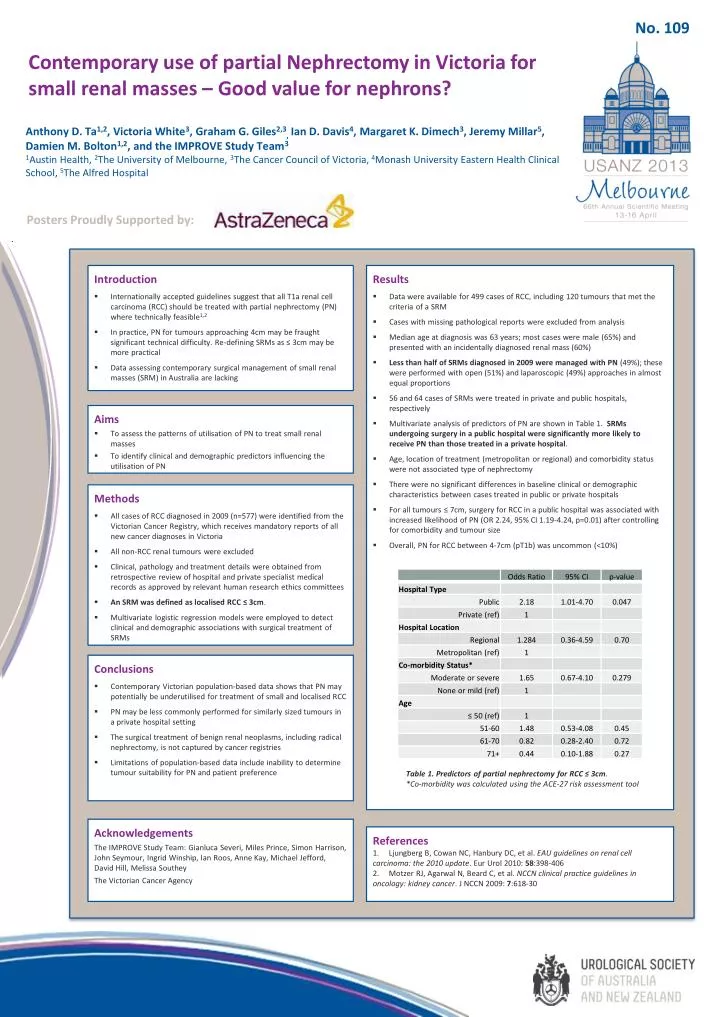
No. 109 Contemporary use of partial Nephrectomy in Victoria for small renal masses – Good value for nephrons? Anthony D. Ta1,2, Victoria White3, Graham G. Giles2,3,Ian D. Davis4, Margaret K. Dimech3, Jeremy Millar5, Damien M. Bolton1,2, and the IMPROVE Study Team3 1Austin Health, 2The University of Melbourne, 3The Cancer Council of Victoria, 4Monash University Eastern Health Clinical School, 5The Alfred Hospital Posters Proudly Supported by: • Results • Data were available for 499 cases of RCC, including 120 tumours that met the criteria of a SRM • Cases with missing pathological reports were excluded from analysis • Median age at diagnosis was 63 years; most cases were male (65%) and presented with an incidentally diagnosed renal mass (60%) • Less than half of SRMs diagnosed in 2009 were managed with PN (49%); these were performed with open (51%) and laparoscopic (49%) approaches in almost equal proportions • 56 and 64 cases of SRMs were treated in private and public hospitals, respectively • Multivariate analysis of predictors of PN are shown in Table 1. SRMs undergoing surgery in a public hospital were significantly more likely to receive PN than those treated in a private hospital. • Age, location of treatment (metropolitan or regional) and comorbidity status were not associated type of nephrectomy • There were no significant differences in baseline clinical or demographic characteristics between cases treated in public or private hospitals • For all tumours ≤ 7cm, surgery for RCC in a public hospital was associated with increased likelihood of PN (OR 2.24, 95% CI 1.19-4.24, p=0.01) after controlling for comorbidity and tumour size • Overall, PN for RCC between 4-7cm (pT1b) was uncommon (<10%) • Introduction • Internationally accepted guidelines suggest that all T1a renal cell carcinoma (RCC) should be treated with partial nephrectomy (PN) where technically feasible1,2 • In practice, PN for tumours approaching 4cm may be fraught significant technical difficulty. Re-defining SRMs as ≤ 3cm may be more practical • Data assessing contemporary surgical management of small renal masses (SRM) in Australia are lacking • Aims • To assess the patterns of utilisation of PN to treat small renal masses • To identify clinical and demographic predictors influencing the utilisation of PN • Methods • All cases of RCC diagnosed in 2009 (n=577) were identified from the Victorian Cancer Registry, which receives mandatory reports of all new cancer diagnoses in Victoria • All non-RCC renal tumours were excluded • Clinical, pathology and treatment details were obtained from retrospective review of hospital and private specialist medical records as approved by relevant human research ethics committees • An SRM was defined as localised RCC ≤ 3cm. • Multivariate logistic regression models were employed to detect clinical and demographic associations with surgical treatment of SRMs • Conclusions • Contemporary Victorian population-based data shows that PN may potentially be underutilised for treatment of small and localised RCC • PN may be less commonly performed for similarly sized tumours in a private hospital setting • The surgical treatment of benign renal neoplasms, including radical nephrectomy, is not captured by cancer registries • Limitations of population-based data include inability to determine tumour suitability for PN and patient preference Table 1. Predictors of partial nephrectomy for RCC ≤ 3cm. *Co-morbidity was calculated using the ACE-27 risk assessment tool Acknowledgements The IMPROVE Study Team: GianlucaSeveri, Miles Prince, Simon Harrison, John Seymour, Ingrid Winship, Ian Roos, Anne Kay, Michael Jefford, David Hill, Melissa Southey The Victorian Cancer Agency References 1. Ljungberg B, Cowan NC, Hanbury DC, et al. EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol 2010: 58:398-406 2. Motzer RJ, Agarwal N, Beard C, et al. NCCN clinical practice guidelines in oncology: kidney cancer. J NCCN 2009: 7:618-30






