Download
1 / 40
410 likes | 612 Views
Hope in the Pipeline I Development of Drugs to Treat TB. IUALTD 2011 - J2J Symposium Daniel Everitt, MD TB Alliance. Development of Drugs to Treat TB Outline of Discussion. Current and historic regimens to treat TB Treatment needs for the future and our historic opportunity

E N D
Hope in the Pipeline IDevelopment of Drugs to Treat TB IUALTD 2011 - J2J Symposium Daniel Everitt, MD TB Alliance
Development of Drugs to Treat TBOutline of Discussion • Current and historic regimens to treat TB • Treatment needs for the future and our historic opportunity • The steps and realities of TB drug development • Specific examples from TB Alliance collaborations • A paradigm shift for drug development • Drugs in the pipeline • Optimism for international collaboration to develop superior treatments for TB 2
1960 Standard Therapy 2 months: R, H, Z, E + 4 months: R, H Rx shortened to 6 months Treatment Evolution for“Drug Sensitive” TB 1950 1970 1980 2005 1946 Strepto-mycin 1st used for TB • 1952 • 1st regimen: • Streptomycin • PAS • Isoniazid (H) 1974 BMRC Trials add R & Z 1998 Rifapentine approved 1963Rifampin (R) discovered 1970 BMRC Trials add R 1961Ethambutol (E) discovered 1954 Pyrazinamide (Z) discovered – but liver toxicity Standard Regimen by 1960s based on 1952 drugs Rx shortened to 9 months Rx lasts from 12-24 months 3
The Burden of Therapy for Multi-drug Resistant TB Example of a typical regimen for MDR-TB • Intensive phase of 6-9 months – aim to directly observe 6 days/week: • Six drug combination, one given by injection • Continuation phase of 18 months: • Four drugs • A patient may need longer therapy if sputum is not clear of TB at month 4 Note: If the patient has HIV, he/she may need to take 3 additional anti-retroviral drugs 4
Current TB Therapy and Unmet Needs • Significant improvements in therapy are needed for all patient populations 5
TB Alliance Founded in 2000 Not-for-profit Product Development Partnership (PDP) headquartered in New York, with offices in Brussels and Pretoria Entrepreneurial, virtual drug development approach Largest portfolio of TB drug candidates in history GOVERNMENTS PHARMA BIOTECH TB Alliance ACADEMIA INSTITUTES FOUNDATIONS 6
TB Alliance Mission Develop new, better treatments for TB that are: faster-acting and less complex compatible with anti-retrovirals for HIV/AIDS coinfection active against drug sensitive and drug resistant strains Ensure that new regimens are affordable, adopted for use, and made widely available Coordinate and act as catalyst for global TB drug development activities 7
FDCs TB Alliance Vision 10 days 2 – 4 months Success will require novel multi-drug combinations 6 – 30 months 8
The need for new TB drugs The need to ensure adherence can put a huge burden on patients Shorter therapies equals > adherence, > cure, < burden on patients, and < emergence of drug resistance 9
What is Needed to Cure a Patient with TB? Effective Medications Adherence to Therapy (DOTS) Health Health Care System to Diagnose TB, Treat, and Confirm Cure Financing of Medications and the Health Care System 10
Classic Phases of Drug Development Discovery Preclinical Clinical ONE approved drug 50 31 19 12 7 4 2 Number of Projects • Global TB Drug Pipeline • (10) (7) (7) (2) (6) (2) 5 Years 1.5 Years 6 Years (Data based on: Brown, D.; Superti-Furga, G. Drug Discovery Today 2003, 8, 1067-1077) 11
New Development Paradigm: Combination testing of novel regimens • Under the new paradigm, the regimen, not an individual drug, becomes the unit of development • New drugs are tested in combinations in clinical trials simultaneously, rather than successively Combination approach reduces time to market by ~3/4ths 12
TB Drug/RegimenDiscovery and Development Process Discovery Single Compound Preclinical Development Phase I EBA Phase II Phase III Compound 1 Compound 2 Drug Candidate Pool Regimen A Compound 3 Regimen B Compound 4 Regimen Identification Compound 5 Regimen C Identification of New Drug Candidates Selection of Potential New Regimens
Drug Development – the Preclinical Phase • Many steps to develop a promising molecule • Safety evaluations typically done in two animal species (e.g. rat and dog) • Pharmacology studies to evaluate efficacy on a relevant endpoint • Aim to find a blood concentration that correlates with the maximum effect 14
Bactericidal Activity of Different Treatment Regimens in the Mouse Log10 CFU in Lungs R= rifampin H= isoniazid Z= pyrazinamide Pa= PA-824 M= moxifloxacin Weeks
Phase 1 Studies – From the lab in to HumanTolerability, pharmacokinetics – often healthy volunteers Example of Phase 1 Study -Single dose pharmacokinetics in healthy volunteers under fed and fasted conditions
Phases 2 and 3 – Evaluate the Effect of the Drug in Patients with the Disease • Some Key Considerations: • Where can we find patients with the disease? • Where can we find investigators who can do a clinical trial with high quality? • What do we measure to show the drug has been effective? 17
Where in the World are Patients with Tuberculosis? www.worldmapper.org 18
Where in the World are Patients with Tuberculosis? www.worldmapper.org 19
Doctors Working in the World www.worldmapper.org 20
How Are We Exposed to the TB Bacteria? Most TB is spread in droplets from the lungs of persons infected with active TB. 22
51 year old Kenyan man with a cough, weight loss, confusion; wife died 3 years earlier with tuberculosis 23
Tuberculosis (Acid Fast Bacillus – “AFB”) from a Sputum Smear Under the Microscope 27
The Tuberculosis Bacteria from a Sputum Sample Growing in a Culture 28
TB Colony Forming Units “CFUs” – Now Countable – from a Diluted Sputum Specimen 29
PA-824: Phase 2 Dose Selection2 week study in patients with TB to choose a dose for later studies RHZE 32
From a Single Drug to a Multi-Drug Regimen to Treat Tuberculosis • Study NC-001 Just Completed • A Phase 2 study of the 3-drug regimen in patients over a 2 week period • PA-824 combined with moxifloxacin and pyrazinamide • Results will be presented at IUATLD Symposium #46, Sunday • Next Step – a 2 month study of the regimen compared to the standard 4 drug combination 33
Implications of Study NC-001 for a Regimen to Treat DS & MDR TB • PaMZ is a well tolerated viable regimen to advance for further testing in both DS & MDR patients sensitive to the regimen • It is safe and feasible to progress from a study of a single drug in patients to a study of that drug in a full regimen as a next step • The mouse model was predictive of the bacterial-killing activity of single drugs and regimens in this short-term human study
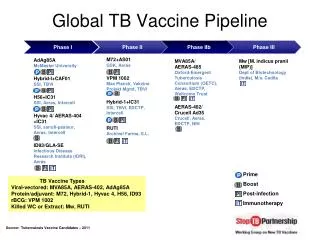
TB Alliance Portfolio Discovery Clinical Development Preclinical Development Lead identification Lead Optimization Target Or Cell-Based Screening Clinical Phase I Clinical Phase II Clinical Phase III TBA-354U. of Auckland/ U. Ill Chicago Moxifloxacin (+ H, R, Z) Bayer Natural Products IMCAS Whole-Cell Hit to Lead Program GSK Mycobacterial Gyrase Inhibitors GSK PA-824 Novartis Preclinical TB Regimen Development JHU/U. Ill Chicago TMC207 Tibotec Moxifloxacin (+ R, Z, E) Bayer TB Drug Discovery Portfolio NITD THPP Series GSK Gyrase B Inhibitors AZ Topoisomerase I Inhibitors AZ/NYMC PA-824/Pyrazinamide Pyrazinamide Analogs Yonsei TMC207/Pyrazinamide Folate Biosynthesis Inhibitors AZ Diarylquinolines Tibotec/U. of Auckland Riminophenazines IMM/BTTTRI Whole-Cell Hit to Lead Program AZ PA-824/TMC207 RNA Polymerase Inhibitors AZ PA-824/Moxifloxacin/Pyrazinamide Energy Metabolism Inhibitors AZ/U. Penn Novel TB regimen development Current first-line TB treatment consists of: isoniazid (H) + rifampicin (R) + pyrazinamide (Z) + ethambutol (E) 35
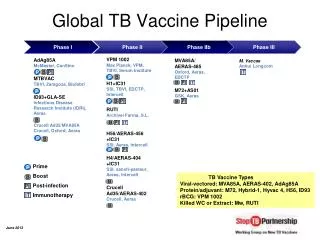
The Global TB Development Pipeline From the Stop TB Partnership Working Group on New Drugs 36
A New Regimen Approved by Regulatory Agencies is Not Enough • How does the new regimen fit in the current WHO/country therapy recommendations? • What will be the barriers to acceptance? • Who are the decision makers? • What work needs to be done before a new regimen is approved? 37
What Countries Want Value Proposition StudyPublished August 2009 • Most stakeholders would welcome treatment shortening as the primary goal. • Unacceptable trade-offs in all countries: • Decreased efficacy • Additional safety concerns or side effects requiring monitoring or expensive adjuvant therapies • Significant drug interactions with other commonly-used drugs (including ARVs) • Unacceptable trade-offs in some countries: • Treatment frequency significantly different from current TB program (e.g., India) • Unavailability in fixed-dose combination (FDC) 38
Our “AAA” Mandate Affordability • Regimens must be sufficiently low cost to be procured in developing countries • Ensured through negotiation of agreements, cost-of-goods considerations in development process Adoption • Public programs and private sector must accept and implement new regimens • Ensured through acceptability studies, engagement with local communities, and direct negotiations with country programs, WHO, and other stakeholders to bring about guideline change Availability • New regimens must be made available to patients in countries that adopt them • Ensured by developing a robust manufacturing and distribution plan with pharmaceutical partners, generics, countries, donors, and other actors 39
40 Years Has Been Too Long to Wait! Shorter, effective, safe regimens for TB therapy are within sight if we work together toward this compelling goal 40