Download

1 / 48
600 likes | 1.87k Views
Blast Injuries. Safwat Abd El Kader MD, FRCS, FICS Professor of Surgery Cairo University Cairo - Egypt. Background. Explosions have the capability to cause multisystem, life-threatening injuries in single or multiple victims simultaneously.

E N D
Blast Injuries Safwat Abd El Kader MD, FRCS, FICS Professor of Surgery Cairo University Cairo - Egypt
Background • Explosions have the capability to cause multisystem, life-threatening injuries in single or multiple victims simultaneously. • These types of events present complex triage, diagnostic, and management challenges for the health care provider. • Explosions can produce classic injury patterns from blunt and penetrating mechanisms to several organ systems, but they can also result in unique injury patterns to specific organs including the lungs and the central nervous system CNS. • Understanding these crucial differences is critical to managing these situations.
Background cont. • The extent and pattern of injuries produced by an explosion are a direct result of several factors including the amount and compositionof the explosive material (eg, the presence of shrapnel or loose material that can be propelled, radiological or biological contamination). • The surrounding environment (eg, the presence of intervening protective barriers). • Thedistance between the victim and the blast. • The delivery method if a bomb is involved. • Any other environmental hazards. • No two events are identical, and the spectrum and extent of injuries produced varies widely.
Background cont. • In many parts of the world, undetonated military incendiary devices such as land mines and hand grenades contaminate the sites of abandoned battlefields. • Such devices cause significant numbers of civilian casualties years and even decades after local hostilities cease. • During wartime, injuries arising from explosions frequently outnumber those from gunshots with many innocent civilians becoming victims.
Background cont. • Much of the challenge facing the care providers is the potential for the sudden creation of large numbers of patients who require extensive medical resources. • This scenario can overwhelm local and hospital resources. Emergency physicians must remain attentive to the possibility and consequences of blast injuries.
Background cont. Once notified of a possible bombing or explosion, hospital-based physicians should consider immediately activating hospital disaster and contingency plans, including preparations to care for anywhere from a handful to hundreds of victims.
Explosive Weights for Potential Improvised Explosive Device (IED) Packages
Pathophysiology • Blast injuries traditionally are divided into 4 categories: primary, secondary, tertiary, and miscellaneous also called quaternary injuries. • A patient may be injured by more than one of these mechanisms. • A primary blast injury is caused solely by the direct effect of blast overpressure on tissue. Air is easily compressible, unlike water. As a result, a primary blast injury almost always affects air-filled structures such as the lung, ear, and gastrointestinal (GI) tract.
Pathophysiology • A secondary blast injury is caused by flying objects that strike people. • A tertiary blast injury is a feature of high-energy explosions. This type of injury occurs when people fly through the air and strike other objects. • Miscellaneous quaternary blast related injuries encompass all other injuries caused by explosions.
Mortality/Morbidity • Mortality rates vary widely between incidents. An analysis of 29 large bombing events between 1966 and 2002 showed 8,364 casualties, including 903 immediate deaths and 7,461 immediately surviving injured. • Immediate death/injury rates were higher for bombings involving structural collapse (25%) than for confined space (8%) and open air detonations (4%).
Mortality/Morbidity • Unique patterns of injury are found in all bombing types. Injury is caused both by direct blast overpressure (primary blast injury) and by a variety of associated factors. • Enclosed-space explosions, including those occurring in busses, and in-water explosions produce more primary blast injury. • Explosions leading to structure collapse produce more orthopedic injuries. • Land mine injuries are associated with a high risk of below- and above-the-knee amputations.
Mortality/Morbidity • Presence of tympanic membrane (TM) rupture indicates that a high-pressure wave (at least 40 kilopascal [kPa], 6 psi) was present and may correlate with more dangerous organ injury. • Theoretically, at an overpressure of 100 kPa (15 psi), the threshold for lung injury, TM routinely ruptures.
CLINICAL History: • If possible, determine what material caused the explosion. • High-order explosives (HEs) • Low-order explosives (LEs)
CLINICAL • If possible, determine the patient's location relative to the center of the explosion. • Because explosions often cause multiple casualties, anticipate activating the hospital or regional disaster plan.
Physical: • Examine lungs for evidence of pulmonary contusion and pneumothorax. • Abdominal injuries from explosions may be occult, and serial examinations are often required.
Physical: • Many experts recommend obtaining a chest radiograph in the presence of isolated tympanic membrane (TM) rupture since this may indicate exposure to significant overpressure. • In a large series of victims of bombings, mostly involving closed spaces, 22% of patients with eardrum perforation had other significant injuries.
Lung Hemorrhage: Pulmonary contusion Hemoptysis Hemothorax Escape of Air: Pneumothorax Pulmonary pseudocyst Arterial gas embolism (AGE)
GI Tract Hemorrhage: Hematoma leading to obstruction Upper or lower GI bleeding Hemoperitoneum Escape of Contents: Mediastinitis Peritonitis
Blast Abdomen 1. Delayed onset > 8-36 hours – more common in submersion • a. Intestinal intra-wall hemorrhages • b. Shearing of local mesenteric vessels • c. Sub-capsular and retroperitoneal hematomas, • d. Fracture of liver and spleen, and testicular rupture 2.Symptoms – exposure + abdominal pain, nausea, vomiting, • hematemesis (rare), rectal or testicular pain and tenesmus 3. Signs – abdominal tenderness, rebound, guarding, absent bowel • sounds, signs of hypovolemia 4. Management – Resect small bowel contusions > 15 mm, • and large bowel contusions > 20 mm
Physical Headaches Dizziness Insomnia Fatigue Uneven gait Nausea Blurred Vision Cognitive Attention difficulties Concentration problems Memory problems Orientation problems Behavioral Irritability Depression Anxiety Sleep disturbances Problems with emotional control Loss of initiative Problems related to employment, marriage, relationships, and home or school management Signs and Symptoms of a Traumatic Brain Injury (TBI)
Ear Middle ear: Ruptured tympanic membrane (TM) Temporary conductive hearing loss Inner ear: Temporary sensory hearing loss Permanent sensory hearing loss
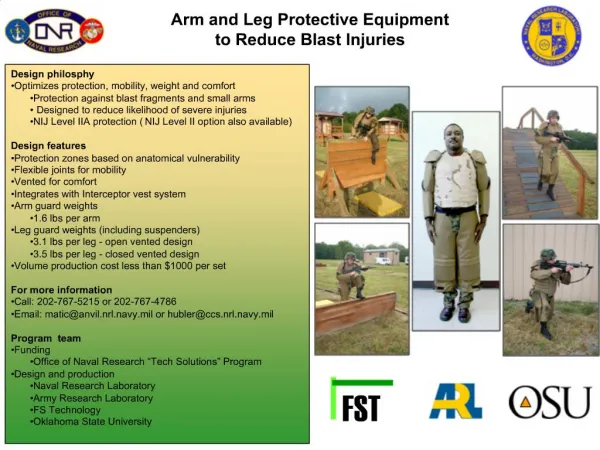
Risk Factors • The closer a casualty is to an explosion, the more likely he will receive primary blast injury (PBI) from the effects of blast overpressure alone, particularly if behind cover and shielded from ballistic trauma. • Personnel in enclosures (buildings, ships, armored vehicles, etc.) are at greater risk, regardless of whether detonation occurred inside or outside the enclosure.
Risk Factors: Personnel treading water are at higher risk for abdominal than thoracic blast injury from underwater explosion. • Fully submerged personnel are at equal risk of combined thoracic and abdominal blast injury, as are personnel in open air, but equivalency occurs at three times distance from explosion underwater compared to open air.
Body armor increases the risk of PBI, but decreases the risk of secondary blast injury from fragments, shrapnel, and debris due to its ballistic protection of vital structures. Tertiary blast injury occurs when the high-velocity blast wind generated by pressure differentials accelerate personnel to tumble along the ground, strike solid objects , or impale themselves on other objects. Secondary and tertiary mechanisms result in conventional blunt and penetrating trauma
Rubber bullet Wael Emad 14 years old boy Died 22 October,2000 PalestineTime magazine