Download
1 / 10
100 likes | 254 Views
PAD Guidelines Changes 2005 >>> 2011 Slides by Omron Healthcare. Published online September 29, 2011 http://content.onlinejacc.org/cgi/content/full/j.jacc.2011.08.023. Updated summary. I. IIa. IIb. III. No Need. Cons ider. Must Do. Rea sonale. Change 1.

E N D
PAD Guidelines Changes2005 >>> 2011Slides by Omron Healthcare Published online September 29, 2011 http://content.onlinejacc.org/cgi/content/full/j.jacc.2011.08.023
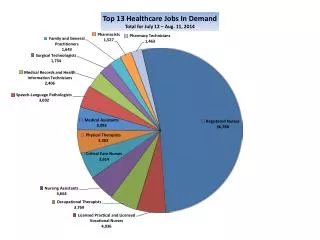
I IIa IIb III NoNeed Cons ider Must Do Rea sonale Change 1 Enlarged Target for Screening 2011 2005 • PAD screening target • Leg symptoms from exertion • Nonhealing wounds • 70 years and older • 50 years and older with a history of • smoking or diabetes. • (Level of Evidence: C) • PAD screening target • Leg symptoms from exertion • Nonhealing wounds • 65 years and older • 50 years and older with a history of smoking or diabetes • (Level of Evidence: B) B * What is level of evidence? See reference page Background of the above change On the basis of a large epidemiologic study*, 21% had either asymptomatic or symptomatic PAD. (*The German Epidemiologic Trial on ABI Study Group)
I IIa IIb III Change 2 More patients will be diagnosed as PAD Increased value of “Pulsewave” function of VP1000+ for better diagnosis of borderline PAD! • The upper cut-off has been increased to 1.4, as in TASCII. • ABI borderline is clearly defined as 0.91-0.9 B 2011 2005 >1.30 1.00-1.29 0.91-0.99 0.41-0.90 0.00-0.40 Noncompressible Normal Borderline??? PAD (mild-moderate) PAD (Severe) Noncompressible Normal Borderline (No change below 0.9) >1.40 1.00-1.40 0.91-0.99 <0.90 Borderline is clearly defined ! The 2005 guidelines are not clearly defined. NoNeed * What is “B”? See reference page Cons ider Must Do Rea sonale
A A Increased importance of Antiplatelet Therapy (esp: Asymptomatic with ABI below 0.9) Change 3 Wider chance for collaboration with antiplatelet pharma companies! Even without symptoms, drug can be prescribed for patients with ABI below 0.9. (See reference page for the pharma list.) 2011 2005 • Antiplatelet therapy is usefulto reduce the risk of MI, stroke, and vascular deathin asymptomatic patients with an ABI 0.9 or less. • Antiplatelet therapy is indicated to reduce the risk of MI, stroke, or vascular death in following patients. • Symptomatic PAD patients with intermittent claudication, ischemia, revascularization, or amputation. • The usefulness of antiplatelet therapy in asymptomatic patients with borderline ABI, is not well established. (should be established) • Antiplatelet therapy is indicated to reduce the risk of MI, stroke, or vascular death in PAD patients NEW More specific NEW
B A A Firmer insistence to Stop Smoking (Smoking cessation program, pharmacological treatment) Change 4 Chance for Omron to collaborate with anti-smoking drug companies! 2005 2011 1. Current or former smokers should be asked at every visit about their smoking. New 2. Patients should be assisted with counselling & in developing a plan for quitting that includes pharmacotherapy and/or smoking cessation program. 3. Current or former smokers should be advised by clinicians to stop smoking and offered behavioral and pharmacotherapy. 4. (If patients can take drugs), one or more of the following should be offered. New New More Specific Current or former smokers should be advised by clinicians to stop it. And should be offered smoking cessation interventions, including behavior modification therapy, nicotine replacement therapy, or bupropion. • Bupropion (GSK:Zyban) • Varenicline (Pfizer: CHANTIX) • Nicotine replacement therapy (Nicotine patch) *Pharma names and products names are not mentioned in the guidelines but for reference.
B B Unchanged but important points Omron promotion 2011 2005 • ABI should be performed on every PAD suspected patient. • Not only specialists, but all clinicians should do ABI! • 2-cuff ABI device is not sufficient. ABI should be measured in both legs at the same time! • We can actively target the DM market with: “Better PAD diagnosis by adding TBI” • For all new patients, ABI should be measured in both legs to confirm the diagnosis of lower extremity PAD and establish a baseline. • The toe-brachial index should be used to establish PAD diagnosis. Targeted patients are those who are clinically suspected as PAD with “noncompressible” ABI value. (usually long-standing DM or advanced age) Unchanged Unchanged
Voice from Dr. Hirsch Dr Alan Hirsch (University of Minnesota, Minneapolis) vice chair of the writing committee chair of the 2005 guidelines • He continues to be concerned that cardiovascular practitioners and primary-care physicians—less than full-time PAD-focused vascular surgeons or interventional radiologists—might not recognize critical limb ischemia as a key cardiovascular syndrome that represents a "slow-burning vascular emergency." • "For this reason, in every community we lose legs, quality of life, and lives," said Hirsch. Source: heartwire
[Reference] What is the level of the evidence? • Multiple study Level A Level B Level C • Limited population but single study • Standard agreed to only experts
[Reference] Antiplatelet pharma Typical/ most prescribed Antiplatelet