Download

1 / 27
270 likes | 391 Views
Competition, Prospective Payment, and Outcomes in Post-Acute Care Markets. Neeraj Sood, Schaeffer Center and School of Pharmacy, USC RAND Corporation. Research Goals. Improve our understanding of: The causes and effects of competition in Post Acute Care (PAC) markets

E N D
Competition, Prospective Payment, and Outcomes in Post-Acute Care Markets Neeraj Sood, Schaeffer Center and School of Pharmacy, USC RAND Corporation
Research Goals • Improve our understanding of: • The causes and effects of competition in Post Acute Care (PAC) markets • How have changes in payment policies both influenced competition and modified the effects of competition on resource use and clinical outcomes
Outline • Policy Context • Research Team • Specific Aims • Hypothesis, Data and Approach
Outline • Policy Context • Research Team • Specific Aims • Hypothesis, Data and Approach
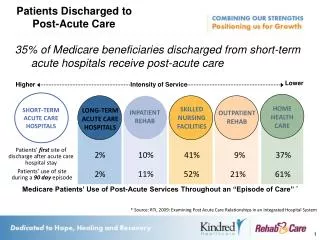
What is Post Acute Care? • Health care services received after discharge from acute care hospital that aim to improve patient functioning and transition from hospital to community • Care can be received in a wide variety of settings including: • Inpatient Rehabilitation Facility (IRF) • Skilled Nursing Facility (SNF) • Long Term Care Hospital (LTCH) • Home Health Care Agencies (HHA)
Post Acute Care is Growing and Large Part of Medicare • In 2006, 2 out of 5 Medicare beneficiaries discharged from hospitals used post acute care • Medicare PAC expenditures more than doubled from 2001 to 2009 • Medicare spent $26.6 billion on PAC in 2001 • Medicare spent $54.4 billion on PAC in 2009
LTCH PPS October, 2002 DRA of 2005 Instituted HHA P4P January, 2007 MMA increased per diem SNF payment October, 2004 SNF PPS July 1, 1998 HHA PPS October 1, 2000 IRF PPS January 1, 2002 MMSEA of 2007 permanently reset IRF 75% rule to 60% December, 2007 HHA IPS October 1,1997 IRF 75% rule (phased in over 4 years) April, 2004 SNF RUG groups increased from 44 to 53 January, 2006 MMSEA of 2007 LTCH 25% rule and moratorium December, 2007 BBRA: SNF PPS Adjusted April 1, 2000 BIPA: SNF PPS Adjusted April 1, 2001 Several Changes in PAC Payment Policy Since 1997 • Move to prospective payment systems (PPSs) for all PAC settings
LTCH PPS October, 2002 DRA of 2005 Instituted HHA P4P January, 2007 MMA increased per diem SNF payment October, 2004 SNF PPS July 1, 1998 HHA PPS October 1, 2000 IRF PPS January 1, 2002 MMSEA of 2007 permanently reset IRF 75% rule to 60% December, 2007 HHA IPS October 1, 1997 (to October 1, 2000) IRF 75% rule (phased in over 4 years) April, 2004 SNF RUG groups increased from 44 to 53 January, 2006 MMSEA of 2007 LTCH 25% rule and moratorium December, 2007 BBRA: SNF PPS Adjusted April 1, 2000 BIPA: SNF PPS Adjusted April 1, 2001 Several Changes in PAC Payment Policy Since 1997 • Move to prospective payment systems (PPSs) for all PAC settings • Several adjustments to PPS and other new payment rules
Other Payment Changes Expected • Current payment system has some issues • Same care in different care settings receive different amount of Medicare payment • Lack of incentives to coordinate care • Patients discharged early from one setting might be readmitted to acute care or receive care in other settings • Several have advocated for bundled acute care and post acute payment • Health care reform bill includes demonstration project
The Composition of PAC Markets is Also Changing • Rapid growth in number of home health care agencies • About 7,000 providers in 2001 • More than 10,000 providers in 2009 • Number of long term care hospitals has also increased rapidly • About 280 long term care hospitals in 2001 • About 430 long term care hospitals in 2009 • Number of IRFs and SNFs have remained stable
How Do Changes in PAC Markets and Payments Impact Medicare? • Little is known about the impact of changes in PAC markets • Have changes in payments influenced entry and exit of providers and competition in PAC markets? • How do changes in number of providers and competition more generally influence patient outcomes and costs? • How have changes in payments and competition affected patient outcomes and costs? • This proposal seeks to address some of these questions
Outline • Policy Context • Research Team • Specific Aims • Data and Approach
Research Team • Neeraj Sood, PhD. (Principal Investigator) • Associate Professor at USC and Senior Economist at RAND • Expertise in empirical economics and health economics • José J. Escarce, M.D., Ph.D (Co-PrincipaI Investigator) • Professor at UCLA and Senior Natural Scientist at RAND • Expertise in post acute care markets and health care financing and organization
Research Team • John Romley, PhD. (Investigator) • Assistant Professor at USC and Economist at RAND • Expertise in industrial organization and competition • Peter Huckfeldt, Ph.D (Investigator) • Associate Economist at RAND • New PhD (will become expert in post acute markets and competition by the end of the project!)
Outline • Policy Context • Research Team • Specific Aims • Hypothesis, Data and Approach
Specific Aims (1 & 2):Examine the Effects of Competition • Examine the effects of competition on resource use and clinical outcomes for PAC episodes among patients discharged from an acute care hospital after a stroke, fracture, or LEJR, and how these effects are mitigated or enhanced by payment policies. • Assess how the effects of competition on resource use and clinical outcomes for PAC episodes differ by care setting.
Specific Aim (3):Examine Determinants of Competition • Describe the variation across geographic market areas and trends over time in PAC competition, and assess the factors that influence these variations and trends, especially changes in PAC payment policies
Outline • Policy Context • Research Team • Specific Aims • Hypothesis, Data and Approach
Specific Aims (1 & 2):Examine the Effects of Competition Study Hypothesis: • Competition increases costs of care but has ambiguous effect on patient outcomes • Switch to PPS reduces effects of competition on costs but effect on patient outcomes is ambiguous • Under PPS, the influence of competition on cost and clinical outcomes is smaller for providers whose payment levels are more constrained
Specific Aims (1 & 2):Examine the Effects of Competition Data: • Medicare claims data from 1996 to 2008 for patients with stroke, hip replacement, & lower extremity joint replacement patients • Mortality data linked to claims data above • Administrative data on nursing home stays (MDS) linked to claims data above • Medicare cost report data to estimate resource use for different providers
Specific Aims (1 & 2):Examine the Effects of Competition Empirical Models: • Outcome Variables • Cost per PAC episode (60, 120, 180 day episodes) • Mortality and/or institutionalization at episode end • Key explanatory variables: • Competition among PAC providers • Competition interacted with payment policy • Cost based versus PPS • Generosity of payments and Medicare share of provider • Covariates include demographics, health status measures, acute hospital and market characteristics
Specific Aims (1 & 2):Examine the Effects of Competition Empirical Models: • Key challenge is accounting for bias due to the fact that competition measures based on actual patient flows might induce spurious correlation between outcomes and competition • Address this concern by constructing competition measures using predicted patient flows that only rely on geographic distribution of patients and providers in a market
Specific Aim (3):Determinants of Competition Study Hypothesis: • More generous Medicare payment for PAC services within a market leads to more competition • Greater demand within a market for PAC services leads to more competition • Lower costs of providing PAC services leads to more competition
Specific Aim (3): Determinants of Competition Data: • Medicare cost report data and provider of service files to estimate number of providers in a given market • Area Resources File, Bureau of Economic Analysis and Medicare claims data to measure demand side factors such as age distribution of population, income, acute care discharges etc • Hospital wage index and Bureau of Labor Statistics data to measure input costs • Data on state policies from a variety of sources
Specific Aim (3): Determinants of Competition Empirical Models: • Outcome Variables • Number of providers • Hirschmann-Herfindahl Index • Key explanatory variables • Payment policy: payment regime and generosity • Demand side factors: population income, age, health status and access to acute care hospitals • Supply side factors: labor costs and rents • Other state policy such as certificate of need laws, minimum staffing rules and Medicaid policy
Potential Policy Implications • Should we promote competition in health care markets? • Understand the extent to which geographic variation in costs and outcomes is influenced by the level of competition • Understand how effects of payment policy changes might vary across markets or regions with different competitive environments
Thank You!Questions? Neeraj Sood, Schaeffer Center and School of Pharmacy, USC RAND Corporation