Download
1 / 27
290 likes | 852 Views
SENIORS Trial: Effect of beta-blockers in elderly patients with impaired renal function. Alain COHEN SOLAL, MD, PhD, FESC Paris. Conflicts of Interest Disclosure.

E N D
SENIORS Trial: Effect of beta-blockers in elderly patients with impaired renal function Alain COHEN SOLAL, MD, PhD, FESC Paris
Conflicts of Interest Disclosure I was the Principal Investigator of the SENIORS Trial for France and member of the Steering Commitee and as such, received honoraria from MENARINI
Prevalence of altered renal function in CHF in the community • CHF with systolic dysfunction (Mc Alister, Circulation 2004) - Cr Cl < 30 ml/min : 16% - Cr Cl 30-59 ml/min: 40% - Cr Cl ≥ 60 ml/min : 44%
Renal dysfunction in HFin the community:insights from the DEVENIR registry N=1 303 Cohen-Solal A et al.HFA 09
Prognostic value of altered renal function in CHF(CHARM) 1.0 4.0 GFRc 3.5 LVEF 0.9 3.0 0.8 > 76 mL/min 2.5 0.7 59 – 76 mL/min Proportion survival Relative risk for mortality 2.0 0.6 44 – 58 mL/min 1.5 0.5 1.0 < 44 mL/min 0.4 0.5 0.0 0.3 0 250 500 750 1,000 1,250 GFRc (mL/min) > 76 59 – 76 44 – 58 < 44 LVEF (%) > 30 26 – 30 20 – 25 < 20 Days Hillege HL, et al. Circulation. 2000;102:203-210.
Background Decreased renal function: - is frequent - is an independent risk factor for HF rehospitalizations and all-cause mortality in patients with heart failure (HF) - often results in restriction to the initiation and titration of HF therapy, that may limit treatment effectiveness especially in the elderly. No study has previously assessed the interaction between beta-blocker response and renal function in elderly HF patients.
Metoprolol and eGFR in MERIT-HF Only patients with LVEF < 35% Young patients Ghali JK et al. (J Cardiac Fail 2009;15:310-318)
Background Decreased renal function: - is frequent - is an independent risk factor for HF rehospitalizations and all-cause mortality in patients with heart failure (HF) - often results in restriction to the initiation and titration of HF therapy, that may limit treatment effectiveness especially in the elderly. No study has previously assessed the interaction between beta-blocker response and renal function in elderly HF patients. The aim of this analysis was to confirm if nebivolol was effective in participants of SENIORS with mild or moderate renal impairment and whether the safety profile was different in these patients.
SENIORS : Inclusion criteria • Age >70 years • NYHA class II-IV. • LVEF was not an entry criterion. • Exclusion criteria : serum creatinine ≥250 micromol/L, contra-indication/intolerance to beta-blockers. • The primary outcome : all cause mortality or cardiovascular hospital admission (time to first event) • Secondary outcomes : all cause mortality, all cause hospital admissions, cardiovascular hospital admissions and cardiovascular mortality
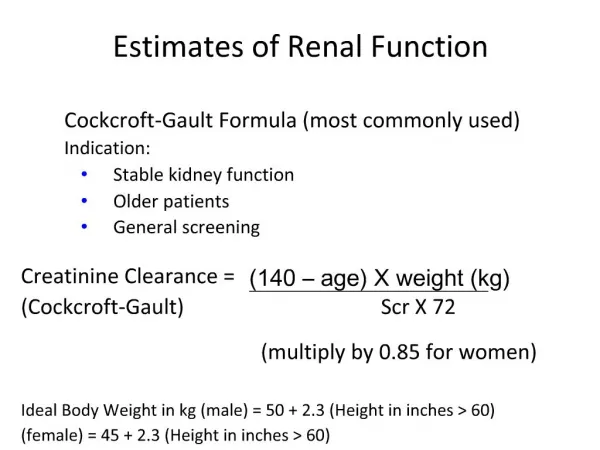
Assessment of renal function Plasma creatinine measured in all SENIORS participants at baseline. Renal function assessment: abbreviated Modification of Diet in Renal Disease (MDRD) formula. The MDRD 4-component equation :eGFR = 186 × [creatinine mg/dl] − 1.154 × [age] − 0.203 × [0.742 if female] × [1.212 if black] GFR was divided into tertiles and broadly corresponds to moderately-impaired, mildly-impaired and normal kidney function, as categorised by the National Kidney Foundation.
Results : baseline variables Age : mean 76.1, SD 4.6 LVEF: mean 36.0%, SD 12.3% Mean GFR for the entire cohort : 65.0 (SD 20.4) ml/min. ≥90 ml/min : 9.9% 60-89 ml/min: 48.1% 30-59 ml/min: 38.9% < 30 ml/min: 3.1%
Baseline variables (1) • ml/min/1.73 m2 • ** across tertiles
Results : Outcome % P<0.001
Hazards ratio : relative effectiveness of nebivolol vs placebo according to eGFR
Discussion • No interaction between eGFR and effectiveness of nebivolol • Class effect ? Experimental study Clinical study
The NO-mediatedvasodilatory effect of Nebivolol on the renal artery Georgescu, Eur J Pharmacol 2005,508:159-66
Effects of Nebivolol and Atenolol on Renal Blood Flow Nebivolol 5: +16+/-22 ml/min Atenolol 50: -86+/-42 ml/min N=10 hypertensives DB, cross over p = 0.02 Van de Borne, High Blood Pressure & Cardiovascular Prevention 2007; 14(3):133-137
Conclusion The efficacy of nebivolol is maintained in patients with mild or moderate renal impairment. In addition nebivolol was safe to use in those with renal dysfunction. Thus, mild to moderate renal dysfunction, even in the elderly, should not present a limitation to the use of nebivolol in heart failure patients