Download
1 / 48
490 likes | 652 Views
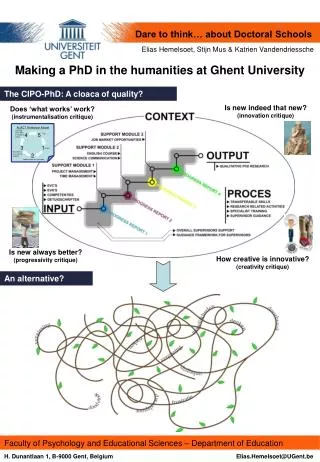
25 years of experience in transgender care at University Hospital Ghent. Thursday November 10, 2011 – Swedish Association for Transsexual Health in Budapest Dr. Griet De Cuypere Department of Sexology and genderproblems University Hospital Ghent - Belgium. “Humanity is divided in 2 categories:

E N D
25 years of experience in transgender care at University Hospital Ghent Thursday November 10, 2011 – Swedish Association for Transsexual Health in Budapest Dr. Griet De Cuypere Department of Sexology and genderproblems University Hospital Ghent - Belgium
“Humanity is divided in 2 categories: - those who believe that it is possible for humanity to be classified in 2 categories, - and those who believe that it is not. The majority of humanity when discussing the distinction ‘men vs. women’ belong to the 1st group.” Citaat van Prof. Dr. P. Cohen - Kettenis
UZGent Genderteam: 1986 • Plastic surgeon: Prof. Dr. Matton • Endocrinologist: Prof. Dr. R. Rubens • Psychiatrist: Dr. G. De Cuypere
UZGent Genderteam: 2011 • Psychiatrists: Dr. G. De Cuypere - coördinator & Dr. G. Heylens • Psychologists: E. Elaut & B. Van Hoorde • Endocrinologist: Prof. Dr. G. T’Sjoen • Plastic surgeon: Prof. Dr. S. Monstrey • Urologist: Prof. Dr. P. Hoebeke • Gynecologist: Dr. S. Weyers • O.R.L. physician: Dr. K. Bonte • Speech-pathologist: Prof. Dr. J. Van Borsel • Dermatologist: Dr. E. Verhaeghen • Lawyer: Prof. Dr. T. Balthazar
UZGent Child GID-team: 2011 • Child - psychiatrist: Dr. K. D’Hondt • Child - psychologists: H. Van den Bossche & J. Laridaen • Endocrinologists: Prof. Dr. R. Craen & Dr. M. Cools
Psychiatrist Psychiatrist Psychiatrist Endocrinologist Psychologist Endocrinologist Endocrinologist Dermatologist Dermatologist Speech pathologist Speech pathologist Plastic surgeon Gynecologist Urologist O.R.L. physician Treatment Procedure Decision for SRS Clinical diagnose Reality diagnose Diagnostic phase Hormonal phase Two years real-life experience
1986 - 2011 • Social evolution • Follow-up research : • Positive predictive factors • Negative predictive factors • Regret-analysis • Medical evolution • Evolution in the law
Social evolution • Last century • Way of thinking : Dichotomic • No difference between terms as female and feminine male and masculine • Current opinions • More genderdiversity • Acceptance of different genderexpression • continuum between man and woman and between maleness and femininity • More attention for kids with genderdysphoria • More attention for reproductive issues
Review on follow-up studies post SRS with regard to regret, suicide and prognosis “Eligibility and Readiness Criteria for Sex Reassignment Surgery: Recommendations for Revision of the WPATH Standards of Care” De Cuypere G & Vercruysse H. International Journal of Transgenderism, 2009, 11, 194-205
Review on follow-up studies post SRS with regard to regret, suicide and prognosis • Analysis of persons who regret: MtF’s: 1 to 1.5 % - FtM’s: less than 1 % Major indicators for regret are: • Inadequate diagnosis • Major psychiatric co-morbidity • Social pressure 2. Suicide The scarce reports do not allow any conclusions to be drawn about the motives
Review on follow-up studies post SRS with regard to regret, suicide and prognosis Negative Predictive Factors: • Late onset, and late request for SRS • Psychiatric co-morbidity and personal instability • Inadequate social functioning indicated by periodical of full dependence on social assistance • Poor support from the patient’s family • Dissatisfaction with secondary sex characteristics at initial assessment • Unsatisfactory surgical results
European Network for the Investigation of Gender Incongruence • Department of Sexology and Genderproblems • University Hospital Gent, Belgium • Griet De Cuypere, Gunter Heylens, Els Elaut • Department of Sex Research and Forensic Psychiatry, • University Medical Center Hamburg-Eppendorf, Germany • Herta Richter-Appelt, Timo Nieder, Susanne Cerwenka • Center of Expertise on Gender Dysphoria, • VU University Medical Centre, Amsterdam, the Netherlands • Peggy Cohen-Kettenis, Baudewijntje Kreukels • Gender Identity Disorder Clinic, Department of Neuropsychiatry, • Rikshospitalet, Oslo, Norway • Ira Haraldsen, Muirne Paap, Lone Nassar
Research questions Do applicants in these four gender identity clinics differ with regard to their GID symptoms and background variables? Do applicants in these four gender identity clinics differ in their psychological functioning / psychiatric co-morbidity? Are there any differences between centers in the percentages of applicants having various gender identity related diagnoses? Are there any differences between centers in the ways the GID-criteria are used to reach a diagnosis?
Diagnostic procedure Sociodemografic and background information: Background interview Gender dysphoria: UGDS Gender Identity Questionnaire Gender Identity Interview Body Image: Body Image Scale Hamburg Drawing Body Scale Appearance: Physical appearance Psychological functioning and psychiatric co-morbidity: Axis I disorders: MINI-plus Axis II – personality disorders: SCID II Psychological functioning: SCL-90, GAF Quality of Life: SF-36 Live as a whole, social function, life events Alcohol and drug use: Drake I and II Diagnostic criteria: DIA and Step 2
Data collection 2007-2010 X exclusions 683 drop-outs MINI and/or SCID N=511 N=174 residual no GID N=330 EO and LO
Characteristics of the sample assessment age: 32.30 ± 11.90 [17-75] (MF 35.16 ± 12.30 vs. FM 28.20 ± 9.88, p<.001) sex ratio Belgium 2.15:1 Germany 1.04:1 The Netherlands 2.27:1 p<.0001 Norway 0.47:1
Conclusions Axis 1 diagnosis occur in 2/3 of the GID population Affective problems are most prevalent and more common compared to GP: current in 27% In up to ¼ of the GID population there is a medium or high suicide risk (past month) Anxiety problems (27%) and substance related problems (15%) have similar prevalences compared to GP Eating problems (0,6%) and psychotic problems (1,5%) are not more common in the GID population Axis 2 diagnosis occurs in comparable prevalence to the GP:12% cluster C > B=A Differences between countries exist for sex ratio, prevalence of axis 1 disorders in general, affective and anxiety disorders GID is a diagnostic entity in its own right
FACULTEIT GENEESKUNDE EN GEZONDHEIDSWETENSCHAPPEN • Results 1) SCL-90 • Significant drop of total score + subscales ANG DEP SEN HOS SOM IN p < 0.05 • More immediately after start of hormones • No difference with reference • population
Effect of hormonal therapy and SRS in patients with genderdysphoria • Genderdysphoria disappears • Is positive on QOL • Symptoms of depression, anxiety, alcohol-and substance abuse, eating disorder decrease • Personality disorders, autism-spectrum disorders, vulnerability for psychosis remain.
Medical evolution - evaluation of own surgical results • FtM • New technique (± 18 years): phalloplastie • All-in-one: a lot of complications, burden for patient • Arm: stigma • Mammectomy: coping with scars • MtF • Epilation by laser – Facial Feminisation surgery (FFS) • Sperm preservation • 1/3 has a low libido after SRS – adaptation to hormonal change • Loss of vaginal depth • Bone problems
Evolutions in the law • New law from September 1, 2007 • After SRS, change in birth-certificate is possible without legal procedure • = simple registration of new gender with certificate of psychiatrist and endocrinologist • Since same-sex marriage is possible, divorce is not anymore a requirement for SRS.
Diagnostic phase – patient • Shared responsability • Patient + MHP: “What is the best solution for your gender issue?” • Persons who don’t want to go through the whole procedure: no problem – we have to take them seriously • For hormonal treatment: pre-requisite to start to live in the preferred gender role from that moment on • Treatment is individualized: • Tempo can be very different • Advise very much against hormonal treatment on their own hook
Diagnostic phase – patient (2) • Issue of procreation is discussed (o.a. preservation of sperm) • Difference is made between • Eligibility criteria • Readiness criteria • (co-morbidity: psychosis, addiction problems, depression, ...) • Treatment of co-morbidity • Stimulation to look for peers – break through isolation
Diagnostic phase – context of patient • Aim: getting more understanding and support = prognostic positive • Parents can have information as much as they wish • Also partner also : if intensive counseling or therapy is needed they are referred • Children: patient – partner and children can receive counseling from our child-psychologist
Hormonal phase - MtF • More attention has been drawn to the adaptation on new hormonal situation - • In some cases: second diagnostic phase is indicated • Reversible • Changes are more gradual - adaptation • Laser-epilation • Evaluation genderdysphoria • Female hormones: different regimes • gel, peroral • Smoke Stop • Voice excercises – or correction • More attention for issues in the new gender role (family, work)
Hormonal phase – FtM • Progestogens: injection to suppress menstruation • Male hormones • Different regimes • Attention for changes in personality (relation-problems) • More attention for real-life experience • Smoke Stop (phalloplasty)
Surgery for Persons with Psychotic Conditions and other Serious Mental Illnesses • Presence of co-existing mental health concerns does not preclude possible changes in gender role or access to hormones or surgery, but need to be managed prior or concurrent with treatment of genderdysphoria. • Effort must be made to improve these conditions with medication and/or psychotherapy before surgery. • Evaluation before surgery. • No surgery should be performed while the patient is actively psychotic.
Surgical phase – MtF • Facial feminisation surgery (FFS) • Feminisation of the face (remove the bossing…) • Rhinoplasty • Attention for orthodontal problems • Vaginoplasty • Implications and complications are discussed • Augmentation mammoplasty • Voice Feminization Surgery • Lipofilling, liposuction…..
Surgical phase – FtM • In our counseling : • Expectations must be realistic • Different regimes : mostly mammectomy and hysterectomy/ovariectomy together • Phalloplasty versus metoïdoplasty • Erection prosthesis • Less frequent surgery • Liposuction • Pectoral implants • Voice Masculinization Surgery
Breast augmentation after 1 year of oestrogens After the start of female sex hormone treatment inmale-to-female transsexual individuals, increase inbreast size usually begins 2-3 months after the start offemale sex hormone treatment, and continues for twoyears. 60 % wishes surgical breastaugmentation
Statement of WPATHWorld Professional Association of transgender health “The WPATH Board of Directors strongly urges the de-psychopathologisation of gender variance worldwide. The expression of gender characteristics, including identities, that are not stereotypically associated with one’s assigned sex at birth is a common and culturally-diverse human phenomenon which should not be judged as inherently pathological or negative. The psychopathologization of gender characteristics and identities reinforces or can prompt stigma, making prejudice and discrimination more likely, rendering transgender and transsexual people more vulnerable to social and legal marginalization and exclusion, and increasing risks to mental and physical well-being. WPATH urges governmental and medical professional organizations to review their policies and practices to eliminate stigma toward gender-variant people.”
Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming PeopleVersion 7 World Professional Association for Transgender Health The original SOC were published in 1979. Previous revisions were in 1980, 1981, 1990, 1998, and 2001.
PURPOSE AND USE OF THE STANDARDS OF CARE To provide safe and effective pathways to achieving lasting personal comfort with their gendered selves in order to maximize their overall health Promote psychological well-being and self-fulfillment
What is new and different? Tone – what professionals need to do rather than emphasis on what the client needs to do Flexibility in the Standards – recognition of unique circumstances More detailed clinical guidelines More than just providing hormones and surgery – it is about promoting overall health and well being New sections – Etherapy, Voice and Communication, Intersex Many references! A clear statement that gender nonconformity is not pathological
Gender nonconformity is not being pathological, yet gender dysphoria is a specific distress that can be alleviated through medically necessary treatment.
Criteria for Hormone Therapy Consolidated gender identity during real-life experience or psychotherapy (min. 3 months) Demonstrable knowledge of what hormones medically can and cannot do and their social benefits and risks 18 years old Progress in mastering other identified problems leading to improving or continuing stable mental health Patient is likely to take hormones in responsible manner Persistent, well-documented gender dysphoria; Capacity to make a fully informed decision and to consent for treatment; Age of majority in a given country (if younger, follow the SOC for children and adolescents); If significant medical or mental concerns are present, they must be reasonably well-controlled. Version 6 Version 7
Criteria for Breast Surgery FtM - Consolidated gender identity during real-life experience or psychotherapy (min. 3 months) - 18 years old - Progress in mastering other identified problems leading to improving or continuing stable mental health - Persistent, well-documented genderdysphoria; - Capacity to make a fully informed decision and to consent for treatment; - Age of majority in a given country (if younger, follow the SOC for children and adolescents); - If significant medical or mental health concerns are present, they must be reasonably well controlled. Version 6 Version 7
Criteria for Breast Surgery MtF Consolidated gender identity during real-life experience or psychotherapy (min. 3 months) 18 years old Progress in mastering other identified problems leading to improving or continuing stable mental health Documentation that breast enlargement for 18 months is not sufficient for comfort is not sufficient for comfort in the social gender role. Persistent, well-documented gender dysphoria; Capacity to make a fully informed decision and to consent for treatment; Age of majority in a given country (if younger, follow the SOC for children and adolescents); If significant medical or mental health concerns are present, they must be reasonably well controlled. Version 6 Version 7 Although not an explicit criterion, it is recommended that MtF patients undergo feminizing hormone therapy (minimum 12 months) prior to breast augmentation surgery. The purpose is to maximize breast growth in order to obtain better surgical (aesthetic) results.
Criteria for Genital Surgery Demonstrated progress in consolidating one’s gender identity Demonstrated progress in dealing with work, family and interpersonal issues resulting in a significantly better state of mental health this implies control of problems such as sociopathy, ,substance abuse, psychosis, suicidality, for instance Legal age of majority Usually 12 months of continuous hormonal therapy for those without a medical contraindication 12 months of successful continuous full time real-life experience. Periods of returning to the original gender may indicate ambivalence about proceeding and generally should not be used to fulfill this criteria If required by the mental health professional, regular responsible participation in psychotherapy throughout the real life experience at a frequency determined jointly by the patient and the mental health professional. Demonstrated knowledge of the cost, required length of hospitalizations, likely complications, and post –surgical rehabilitation requirements of various surgical approach and awareness of different competent surgeons. Persistent, well documented gender dysphoria; Capacity to make a fully informed decision and to consent for treatment; Age of majority in a given country; If significant medical or mental health concerns are present, they must be well controlled; 12 continuous months of hormone therapy as appropriate to the patient’s gender goals (unless the patient has a medical contraindication or is otherwise unable or unwilling to take hormones); 12 continuous months of living in a gender role that is congruent with their gender identity (for metoidioplasty or phalloplasty in FtM patients and for vaginoplasty in MtF patients; not for gonadectomy) Although not an explicit criterion, it is recommended that these patients also have regular visits with a mental health or other medical professional. Version 6 Version 7