Download
1 / 25
300 likes | 930 Views
Joint Hospital Surgical Grandround. Management of Toxic Multinodular Goiter - R ole of surgery. Shi LAM Queen Mary Hospital. Hyperplastic (Grave’s) Non-hyperplastic (Plummer’s) Solitary toxic nodule Toxic multinodular goiter Two major causes (> 80%) of hyperthyroidism worldwide.

E N D
Joint Hospital Surgical Grandround Management of Toxic Multinodular Goiter - Role of surgery Shi LAM Queen Mary Hospital
Hyperplastic (Grave’s) Non-hyperplastic (Plummer’s) Solitary toxic nodule Toxic multinodular goiter Two major causes (> 80%) of hyperthyroidism worldwide “..two distinct types of thyroid intoxication…” – H.S Plummer 1913
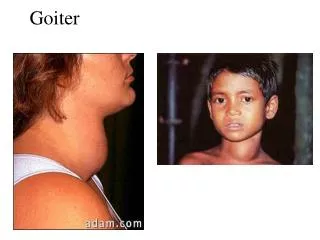
Multinodular Goiters (MNG) • Commonly adopted definition • thyroid volume > 20ml • nodular lesions > 5 – 10mm • Prevalence determined by iodine intake • palpation: 3 – 5% • USG screening: 10 - 50% • endemic in regions of low iodine intake • risk factors: age, female, parity, smoking, obesity
Hong Kong is a region of borderline iodine deficiency • Chinese Nutrition Society Recommendation • adolescent / adult : 150 ug / day • pregnant / lactating women: 250 ug / day • upper limit 1000 ug/day • Center for food safety report 2011 • median daily food iodine content 44 ug/day • 59% of population has iodine intake < 50 ug / day • iodine rich food: seaweed > crustaceans > eggs > milk > fish • iodine scarce food: grains, meat, vegetable, tea / coffee
Natural history – nodule growth • Alexander et al. Ann Intern Med 2003 • USG follow-up of 330 benign nodules • 39% nodules increase volume by 15% in 35 months • cystic nodules tend to remain static • age, gender and TSH level were not predictive of nodule growth • Papini et al. J Clin Endocrinol Metab. 1998 • 45% increase volume, 25% in nodule number in 5 years
Natural history - thyrotoxicosis • Prospective cohorts • Elte et al. Postgrad Med J 1990 • Wiener et al. Clin Nucl Med. 1979 • 158 euthyroid MNG patients with autonomous functioning thyroid • mean follow-up 4 – 12.2 years • 10% patients develop thyrotoxicosis • Factors associated with hyperthyroidism • older age • hyperfunctional nodules size > 3cm • autonomously functioning thyroid volume > 16ml
Spectrum & course of Plummer’s disease Plummer’s disease
Spectrum & course of Plummer’s disease Toxic multinodular goiter
Spectrum & course of Plummer’s disease Iodine exposure
Management of toxic MNG • Goals • correct dysfunction – mass / thyrotoxicosis • exclude / treat malignancy • Options • medical • radio-active iodine • surgery • percutaneous ablations
Overt thyrotoxicosis in toxic MNG • Preferred treatment options • surgery • total / near-total thyroidectomy • immediate restoration of euthyroidism • retrosternal goiters, weight > 90g • <1% retreatment rate • <2% permanent recurrent laryngeal nerve injury • <2% permanent hypoparathyroidism • contraindications: pregnancy (1st and 3rd trimester)
Overt thyrotoxicosis in toxic MNG • Preferred treatment options • 131I • avoids surgical / anaesthetic risk • euthyroidism: 3 months – 60%, 6 months – 80% • hypothyroidism: 1 year – 3%, 24 years – 64%; • 40% size reduction • contraindications: • lactating • pregnant / planning pregnant in 6 months
Overt thyrotoxicosis in toxic MNG • Other treatment options • Anti-thyroid medications • does not induce remission • for patients not fit for surgery, limitted life expectancy • Percutaneous ablation (ethanol / radio-frequency / high intensity focused ultrasound ) • lack of long-term experience
Subclinical thyrotoxicosis • Common in toxic multinodular goiter • Porterfield et al. World J Surg 2008 • 438 / 586 (82%) patients with toxic nodular goiter • Long-term consequence • Sawin et al. NEJM 1994 • prospective cohort of 2007 subjects > 60 years old • follow-up: 10 years • subjects with subclinical hyperthyroidism (TSH < 0.1 mU/L) have 3-fold increased risk in developing atrial fibrillation
Risk of malignancy • Incidental carcinoma in toxic multinodular goiter: • Review by Pazaitou et al. Horm Metab Res 2012 • 7 retrospective cohorts of toxic nodular goiter • 1611 subjects • Cancer in 1.6 – 8.8% • Microcarcinoma (<10mm): 35 – 88% of tumors • Excellent prognosis compared with euthyroid patients • QMH(unpublished) • Toxic multinodular goiter operated for non-suspicious causes • Excluded FNAC confirmed or suspicious nodules • 16/178 (9%) found to have carcinoma • 15 papillary carcinoma, 1 Hurthle cell carcinoma • Mean diameter 12mm
Risk of malignancy • ? Clinical significance • higher reported prevalence due to more detailed pathological examination ? • hyperthyroidism not previously identified as risk factors for manifesting carcinoma of thyroid • ? Pre-operative risk stratification • cold nodules on scintigraphy • family history • exposure to neck irradiation • USG findings • > 50% carcinomas found outside of “dominant” / “cold” nodules
Summary • Toxic multinodular goiter is the manifesting stage of a chronic process of hyperplasia and acquisition of automaticity in the thyroid gland. • Hyperthyroidism, overt or subclinical, is an indication for definitive interventions, in the form of thyroidectomy or radio-active iodine ablation. • In the absence of suspicion of malignancy, surgery is probably still a “safer offer” in younger patients in view of the accumulated life-time risk for an incidental carcinoma to progress into a manifesting cancer.
Acknowledgement Dr. Brian Lang