Download
1 / 12
150 likes | 644 Views
Varicose Veins. Dr. Belal Hijji, RN, PhD April 4, 2012. Learning Outcomes. At the end of this lecture, students will be able to Define and describe varicose veins. Describe the prevalence and risk factors of varicose veins. Discuss the clinical picture and diagnosis of varicose veins.

E N D
Varicose Veins Dr. Belal Hijji, RN, PhD April 4, 2012
Learning Outcomes At the end of this lecture, students will be able to • Define and describe varicose veins. • Describe the prevalence and risk factors of varicose veins. • Discuss the clinical picture and diagnosis of varicose veins. • Describe the medical and nursing management of varicose veins.
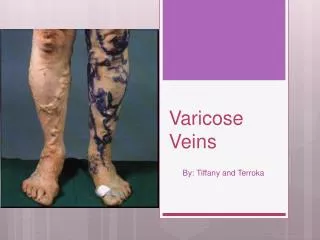
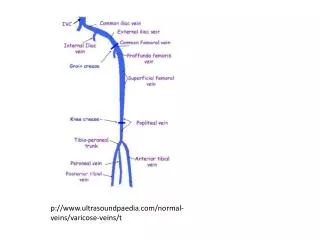
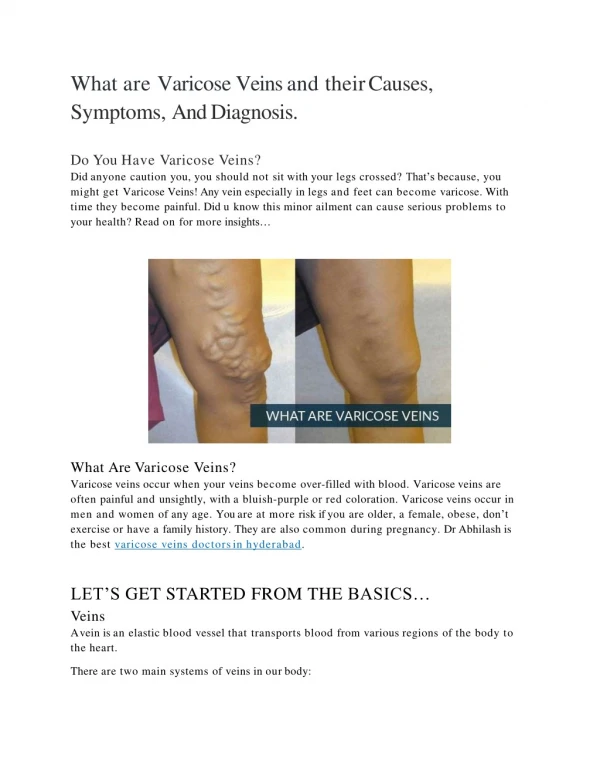
Definition • Varicose veins are abnormally dilated, tortuous, superficial veins caused by incompetent venous valves (see Fig. 1). Most commonly, this condition affects the lower extremities, the saphenous veins (Slide 2), and may occur in the esophagus. Fig. 1: Competent valves showing blood flow patterns when the valve is open (A) and closed (B), allowing blood to flow against gravity. (C) With faulty or incompetent valves, the blood is unable to move toward the heart.
Prevalence And Risk Factors For Developing Varicose Veins • Varicose veins affects about 60% of the adult population in America. In KSA, the prevalence of chronic venous insufficiency (of which varicose veins is just one class) was found to be 45.6% (50% among female and 25% among male) (Bawakid et al. 2005). • The risk for developing varicose veins is associated with increased age, gender, those with occupations requiring prolonged standing, such as salespeople, hair stylists, teachers, nurses, ancillary medical personnel, construction workers, family history, pregnancy (hormonal effects, increased pressure).
Clinical Manifestations • The patient maybe asymptomatic. However, the patient may have dull aches, muscle cramps, increased lower legs muscle fatigue, ankle edema and a feeling of heaviness of the legs. Nocturnal cramps are common. When deep venous obstruction results in varicose veins, patients may have edema, pain, pigmentation, and ulcerations. Susceptibility to injury and infection is increased.
Assessment and Diagnostic Findings • Duplex scanning (see figure below) has become the 'gold standard' for confirming reflux and demonstrating anatomy in cases of lower limb venous disease.
Prevention of Varicose Veins • Activities that cause venous stasis should be avoided. These include wearing tight socks or a constricting panty girdle (Rt. Figure), crossing the legs, and sitting or standing for long periods. • Changing position frequently, elevating the legs when tired, and walking (if not contraindicated), rather than using an elevator, promote circulation. Swimming is also good exercise for the legs. Patients should use knee-high stockings (Middle Figure) than thigh-high stockings (Lt. Figure). The overweight patient should reduce his weight.
Medical Management • Sclerotherapy. In this procedure, small- and medium-sized varicose veins are injected with a chemical that scars and closes those veins. In a few weeks, treated varicose veins should fade. After the injection, elastic compression bandages are worn for approximately 5 days. Elastic compression stockings are then worn for an additional 5 weeks. Patients are encouraged to perform walking activities as prescribed to maintain blood flow in the leg. • Laser surgeries. Laser treatments are used to close off smaller varicose veins and spider veins. Laser surgery works by sending strong bursts of light onto the vein, which makes the vein slowly fade and disappear. No incisions or needles are used.
Medical Management • Vein stripping. This procedure involves removing a long vein through small incisions. This is an outpatient procedure for most people. Removing the vein won't affect circulation in your leg because veins deeper in the leg take care of the larger volumes of blood.
Nursing Management • Postoperatively, bed rest is maintained for 24 hours. Subsequently, the patient begins walking every 2 hours for 5 to 10 minutes. • Elastic compression stockings are used to maintain compression of the leg. They are worn continuously for about 1 week postop. • The nurse assists the patient to perform exercises and move the legs. The foot of the bed should be elevated. • Standing still and sitting are discouraged.
Promoting Comfort and Understanding • The nurse administers analgesics to help patients move affected extremities more comfortably. Dressings are inspected for bleeding, particularly at the groin, where the risk of bleeding is greatest. • The nurse is alert for reported sensations of “pins and needles.” Hypersensitivity to touch in the involved extremity may indicate a temporary or permanent nerve injury resulting from surgery, because the saphenous vein and nerve are close to each other in the leg. • The patient may shower after the first 24 hours. The patient is instructed to dry the incisions well with a clean towel without rubbing. Application of skin lotion is to be avoided until the incisions are completely healed to decrease the chance of developing an infection.