Download
1 / 52
520 likes | 667 Views
Alex Neuro 2014. MAGNETIC RESONANCE SPECTROSCOPY VERSUS STEREOTACTIC BIOPSY FOR INTRA-AXIAL BRAIN LESIONS. Assistant Lecturer Of Neurosurgery, Alexandria, Egypt. Presented By. Ahmed Belal. Intra-axial brain lesions could be neoplastic or non-neoplastic.

E N D
Alex Neuro 2014 MAGNETIC RESONANCE SPECTROSCOPY VERSUS STEREOTACTIC BIOPSY FOR INTRA-AXIAL BRAIN LESIONS Assistant Lecturer Of Neurosurgery, Alexandria, Egypt Presented By Ahmed Belal
Intra-axial brain lesions could be neoplastic or non-neoplastic. Some non-neoplastic brain lesions can mimic the neoplastic lesions clinically, radiologically and sometimes histopathologically. And this may lead to misdiagnosis and hence mismanagement.
MRS is usually used as a complement to conventional MRI to improve the diagnosis of intra-axial parenchymal brain lesions
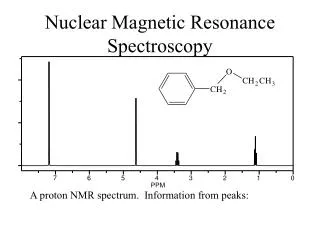
Magnetic Resonance Spectroscopy (MRS) is based on the chemical shift properties of the atom. When a tissue is exposed to an external magnetic field, its nuclei will resonate at a frequency (f). The most common nuclei used for MRS are protons (H1) mainly because of its high sensitivity and abundance.
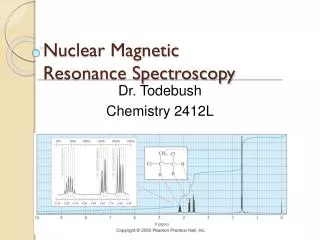
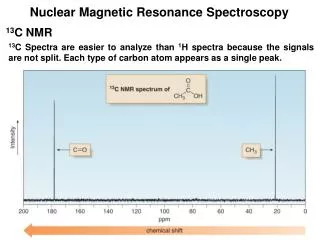
The MR spectrum is represented by: • (x) axis that corresponds to the metabolite frequency in ppm according to the chemical shift • (y) axis that corresponds to the peak amplitude Each metabolite is identified by the position of its peak on a frequency scale (the chemical shift)
N-acetylaspartate(NAA) : • Peak of NAA is the highest peak assigned at 2.02 ppm. • It is a marker of neuronal and axonal viability and density . • Absence or decreased concentration of NAA is a sign of neuronal loss or degradation
Choline (Cho): • Its peak is assigned at 3.22 ppm • Cho is a marker of cellular membrane turnover (phospholipids synthesis and degradation) reflecting cellular proliferation • In tumors, Cho levels correlate with degree of malignancy
Creatine (Cr) : • The peak of Cr spectrum is assigned at 3.02 ppm • Cr is a marker of intracellular metabolism. • Concentration of Cr is relatively constant. Therefore it is used as an internal reference for calculating metabolite ratios. • In brain tumors, there is a reduced Cr signal
Lactate (Lac) : • The peak of Lac is a doublet • Lac is a product of anaerobic glycolysis so its concentration increases under anaerobic metabolism such as cerebral ischemia. • Lac also accumulates in tissues with poor washout such as cysts, normal pressure hydrocephalus, necrotic and cystic tumors.
Lipids (Lip) • Lipid peaks can be seen when there is cellular membrane breakdown or necrosis such as in metastases or primary malignant tumors.
Myoinositol (Myo) : • Myois considered a glial marker because it is primarily synthesized in glial cells, almost only in astrocytes • Elevated Myo occurs with proliferation of glial as found in inflammation , gliosis and in Alzheimer’s disease
Clinical applications of MR spectroscopy
Differentiation between neoplastic and non- neoplastic lesions • The typical MRS spectrum for a brain tumor is one of high level of Cho, low NAA and minor changes in Cr • Cho elevation is usually evidenced by increase in Cho/NAA or Cho/Cr ratios, rather than its absolute concentration • Absence of NAA in an intra-axial tumor generally implies an origin outside of the central nervous system (metastasis) or a highly malignant tumor that has destroyed all neurons in that location.
Grading of cerebral gliomas • Distinguishing between primary brain tumors and metastases • Distinguishing radiation necrosis from tumor recurrence
This study was conducted on 27 patients presented to the Neurosurgery Department at Alexandria Main University Hospital.
All patients were subjected to: • Complete history taking. • Full clinical examination. • Pre-operative investigations: • Routine laboratory investigations. • Contrast enhanced Computed Tomography (CT) scan of the brain • Contrast enhanced Magnetic Resonance Imaging (MRI) of the brain. • Magnetic Resonance Spectroscopy (MRS) of the lesion Either single or multivoxel MRS was used with short and long TE
Surgical techniques: • Stereotactic biopsy using Leksell Stereotactic System. • Histopathologicalexamination • using appropriate stains including immunostains
The preoperative MRS suggested diagnosis was Neoplasticbrain lesions in 15 (56%) cases Non-neoplasticbrain lesions in 12 (44%) cases
The most common MRS diagnosis was High grade gliomas, 7 cases (26%)
The histopathological diagnosis was Neoplastic lesions in 17 cases (63%) Non-neoplastic lesions in 10 cases (37%)
The commonest diagnosis following stereotactic biopsy was Glioblastomamultiforme(GBM) , (WHO grade IV), 10 cases (37%) The commonest diagnosis of the non-neoplastic cases was Brain abscess, 3 cases (11%)
Correlation between the preoperative diagnosis by MRS and Histopathoplogicaldiagnosis following Stereotactic Biopsy for Differentiation between Neoplastic and Non-neoplastic brain lesions revealed Matching In 25 Out Of 27 Cases Sensitivity 88% Specificity 100%
One case was diagnosed by MRS as a Neuroglial cyst but the histopathological diagnosis of the stereotactic biopsy was Cystic astrocytoma. Another case was diagnosed by MRS as an Abscessbut the histopathological diagnosis of the stereotactic biopsy was Glioblastomamultiforme(WHO grade IV). However, the convential MRI was lacking the DWI/ADC map, which is diagnostic for brain abscess
Correlation between the preoperative diagnosis by MRS and Histopathoplogical diagnosis following Stereotactic Biopsy For Grading of Gliomas (12 cases ) revealed Matching in10out of the12cases Sensitivity 89% Specificity 67%
Case 1 Rt thalamic lesion
The MRS shows : • Increassed Cho/Cr • Increased Cho/NAA • Decreased NAA/Cho ratio • Features suggestive of high grade glioma
Histopathological diagnosis was GBM (WHO IV)
Case 2: Rt thalamic cystic lesion
The MRS from within the center of the lesion revealed • very prominent Lip peak (block arrow) • very prominent peak of succinate (long arrow) • Small amino acid peak (arrow head) • Lac peak (right angle arrow) • Such findings were typical for an anaerobic abscess
Case 3: Rt lenticular cystic lesion
The initial MRS was in favor of a Neuroglial Cyst. However, after subsequent revision of the MRS findings it revealed Increased Cho/Cr, Cho/NAA ratios Decreased NAA/Cho ratio Features are matching with a Neoplastic lesion
Case 4: Multiple enhancing brain lesions
The MRS shows Increased Cho/Cr , Cho/NAA ratios Decreased NAA/Cho, NAA/Cr ratios, Lip and Lac peaks are seen Detectable Glx peak multicentricneoplastic lesion; Primary CNS lymphoma was the prime diagnosis
Case 5: Bithalamic ill defined lesion
The MRS shows Preserved NAA and NAA/Cho ratio Decreased NAA/Cr ratio Increased Cr peak Detectable Lac peak MRS features of Encephalitis
Case 6 Multiple lesions
The MRS shows High Cho/Cr , High Cho/NAA Decreased NAA/Cho Lactate Peak Is Prominent (White Arrow) Small Lip Peak was also detected (block Arrow). Normal Spectroscopic findings in the peritumoral region Overall data were matching with Metastatic Lesions
Case 7: Lt deep parietal enhancing lesion
The initial MRS was in favor of Brain Abscess. However, after subsequent revision of the MRS findings it revealed Marked increase in Cho/Cr and Cho/NAA ratios Prominent lip peak Which were in favor of High Grade Glioma