Download
1 / 1
10 likes | 205 Views
BACTERIAL CO-INFECTIONS IN PATIENTS WITH FUNGAL BLOODSTREAM INFECTIONS ARE FREQUENT , BUT DO NOT INCREASE MORTALITY N . Kulkova * , J. Sokolova, S. Spanik , A. Demitrovicova , L. Drgona , B. Rudinsky , M. Huttova ,

E N D
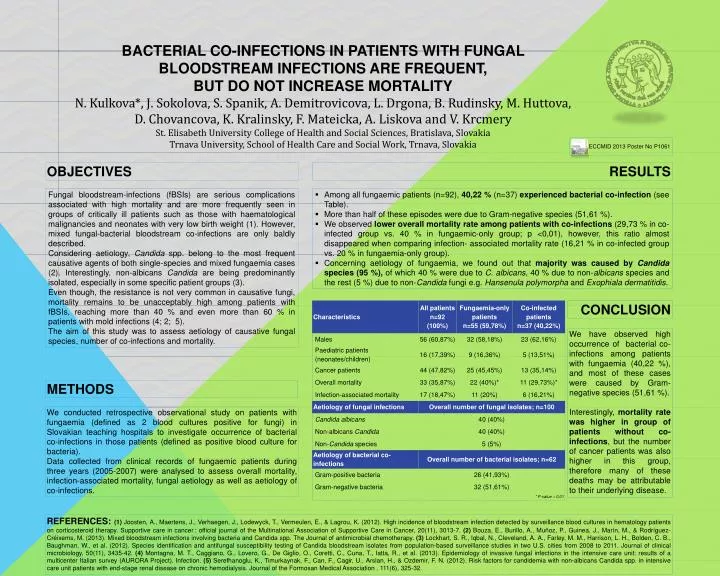
BACTERIAL CO-INFECTIONS IN PATIENTS WITH FUNGAL BLOODSTREAM INFECTIONS ARE FREQUENT, BUT DO NOT INCREASE MORTALITY N. Kulkova*, J. Sokolova, S. Spanik, A. Demitrovicova, L. Drgona, B. Rudinsky, M. Huttova, D. Chovancova, K. Kralinsky, F. Mateicka, A. Liskova andV. Krcmery St. Elisabeth University College of Health and Social Sciences, Bratislava, Slovakia Trnava University, School of Health Care and Social Work, Trnava, Slovakia ECCMID 2013 Poster No P1061 OBJECTIVES RESULTS • Among all fungaemic patients (n=92), 40,22% (n=37) experienced bacterial co-infection (seeTable). • More than half of these episodes were due to Gram-negative species (51,61%). • We observed lower overall mortality rate among patients with co-infections (29,73% in co-infected group vs. 40% in fungaemic-only group; p <0,01), however, this ratio almost disappeared when comparinginfection- associated mortality rate (16,21% in co-infected group vs. 20% in fungaemia-only group). • Concerning aetiology of fungaemia, we found out that majority was caused by Candida species (95%), of which 40% were due to C. albicans, 40% due to non-albicans species and the rest (5%) due to non-Candida fungi e.g. Hansenulapolymorphaand Exophialadermatitidis. Fungal bloodstream-infections (fBSIs) are serious complications associated with high mortality and are more frequently seen in groups of critically ill patients such as those with haematological malignancies and neonates with very low birth weight (1). However, mixed fungal-bacterial bloodstream co-infections are only baldly described. Considering aetiology, Candida spp. belong to the most frequent causative agents of both single-species and mixed fungaemia cases (2). Interestingly, non-albicans Candida are being predominantly isolated, especially in some specific patient groups (3). Even though, the resistance is not very common in causative fungi, mortality remains to be unacceptably high among patients with fBSIs, reaching more than 40 % and even more than 60 % in patients with mold infections (4; 2; 5). The aim of thisstudy was to assess aetiology of causative fungal species, number of co-infections and mortality. CONCLUSION We haveobserved high occurrence of bacterial co-infections among patients with fungaemia (40,22%), and most of these cases were caused by Gram-negative species (51,61 %). Interestingly,mortality rate was higher in group of patients without co-infections, butthe number of cancer patients was also higher in this group, therefore many of these deaths may be attributable to their underlying disease. METHODS We conducted retrospective observational study on patients with fungaemia (defined as 2 blood cultures positive for fungi) in Slovakian teaching hospitals to investigate occurrence of bacterial co-infections in those patients (defined as positive blood culture for bacteria). Data collected from clinical records of fungaemic patients during three years (2005-2007) wereanalysed to assess overall mortality, infection-associated mortality, fungal aetiology as well as aetiology of co-infections. REFERENCES: (1)Joosten, A., Maertens, J., Verhaegen, J., Lodewyck, T., Vermeulen, E., & Lagrou, K. (2012). Highincidenceofbloodstreaminfectiondetected by surveillance bloodcultures in hematologypatients on corticosteroidtherapy. Supportivecare in cancer : officialjournaloftheMultinationalAssociationofSupportiveCare in Cancer, 20(11), 3013-7.(2)Bouza, E., Burillo, A., Muñoz, P., Guinea, J., Marín, M., & Rodríguez-Créixems, M. (2013). Mixedbloodstreaminfectionsinvolvingbacteria and Candida spp. TheJournalofantimicrobialchemotherapy. (3)Lockhart, S. R., Iqbal, N., Cleveland, A. A., Farley, M. M., Harrison, L. H., Bolden, C. B., Baughman, W., et al. (2012). Species identification and antifungalsusceptibilitytestingof Candida bloodstreamisolatesfrompopulation-based surveillance studies in two U.S. citiesfrom 2008 to 2011. Journalofclinicalmicrobiology, 50(11), 3435-42. (4)Montagna, M. T., Caggiano, G., Lovero, G., DeGiglio, O., Coretti, C., Cuna, T., Iatta, R., et al. (2013). Epidemiologyofinvasivefungalinfections in theintensivecareunit: resultsof a multicenterItaliansurvey (AURORA Project). Infection. (5)Serefhanoglu, K., Timurkaynak, F., Can, F., Cagir, U., Arslan, H., & Ozdemir, F. N. (2012). Risk factorsforcandidemiawithnon-albicans Candida spp. in intensivecareunitpatientswithend-stagerenaldisease on chronichemodialysis. JournaloftheFormosanMedicalAssociation.111(6), 325-32.