Download
1 / 30
300 likes | 412 Views
Investigation of the Increased Rate of False Positive Results Using an Oral Mucosal Rapid HIV Test. Centers for Disease Control and Prevention Minnesota Department of Health New Jersey Department of Health & Senior Services Wisconsin Division of Public Health. Background.

E N D
Investigation of the Increased Rate of False Positive Results Using an Oral Mucosal Rapid HIV Test Centers for Disease Control and Prevention Minnesota Department of Health New Jersey Department of Health & Senior Services Wisconsin Division of Public Health
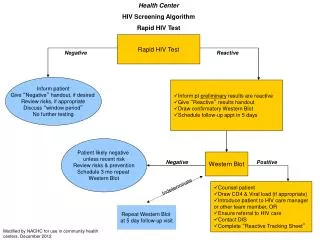
Background • University of Minnesota demonstration project • Finger stick and oral mucosal transudate (OMT) rapid HIV tests • Incidence of Type I, II discordant results • Factors associated with discordant results • OMT test Clinical Laboratory Improvement Amendment (CLIA) waived • OMT test was scheduled for launch end- August 2004
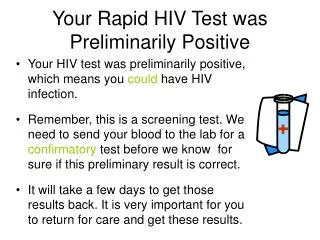
Preliminary Data • July 2002 – April 14, 2004: • 2,022 individuals tested • 7 OMT false positives (0.35%) • April 15, 2004 – July 22, 2004: • 266 individuals tested • 15 OMT false positives (5.6%) • 5-20% false positive rates reported in community trials
Investigation • Started with Epi Aid investigation on invitation of Minnesota Department of Health • Developed into multi-state investigation • Key component is case control study
Objectives • Determine rate of false positive OMT rapid HIV tests • Determine factors associated with false positive OMT tests • Host immunological factors • Medical conditions • Interfering substances
Sites and Duration • New Jersey, Wisconsin, Minnesota • New Jersey: • Robert Wood Johnson (New Brunswick) • Henry J. Austin (Trenton) • NJCRI • Bergen County • Atlantic City Health Department • East Orange Health Department • 4 months
Study Population • Cases (n=150): • 50 to be enrolled in NJ • Reactive OMT rapid test • Non-reactive finger-stick rapid test • Exclude HIV positive individuals after confirmatory HIV test result • Controls (n=450): • 150 to be enrolled in NJ • Non-reactive OMT rapid test • Non-reactive finger-stick rapid test • Exclude HIV positive individuals after confirmatory HIV test result • Exclude temporally related controls after case confirmed to be HIV positive
Eligibility Criteria • 18 yrs or older • No previous HIV diagnosis • No history of antiretroviral therapy • No HIV vaccine
Methods • Phase I • Conduct fingerstick and OMT rapid HIV tests • Administer questionnaire • Collect serum and OMT specimens • Perform HIV confirmatory testing on serum and OMT • Analyze test devices • Bank specimens for Phase II • If sufficient OMT false positives, continue study
Methods • Phase II • Continue recruitment of cases and controls • Perform all other laboratory tests • Analyze data using multivariate logistic regression • Continue device analysis
Laboratory Tests • Serum: • Hepatitis A, B, C • Rheumatoid factor • EBV • Quantitative HCG pregnancy test • ANA • RPR • Protein electrophoresis • Gel electrophoresis with immunofixation for Ig estimation • HSV I and II • CMV • Oral fluid: • Confirmatory HIV EIA/WB • Immunoglobulin estimation- protein electrophoresis
Analysis of Test Devices • Microscopy or other physical methods to characterize false positive results • Ship devices to CDC
Enrolling a Case • Administer written consent for rapid tests (stage 1) • Perform fingerstick and OMT rapid tests • Assess if potential case • Non-reactive fingerstick result • Reactive OMT result • Check for eligibility • Administer written consent (stage 2) • Administer questionnaire • Collect blood and OMT specimens • Ship specimens and devices to CDC
Enrolling a Control • Administer written consent for rapid tests (stage 1) • Perform fingerstick and OMT rapid tests • Assess if potential control • Non-reactive fingerstick result • Non-reactive OMT result • Check for eligibility • Administer written consent (stage 2) • Administer questionnaire • Collect blood and OMT specimens • Ship specimens and devices to CDC
Clinic Flow Recruit CASE: Reactive OMT Non-reactive fingerstick Recruit next 3 consecutiveCONTROLS: Non-reactive OMT Non-reactive fingerstick
Questionnaire • Hand-held devices • Enter • subject ID, location, date and time • fingerstick and OMT device lot numbers • fingerstick and OMT test results • Go through all questions • Confirm subject ID at end of interview
Specimens and Devices • Specimens • 37 mL venipuncture whole blood • 3 serum separator tubes: red top/tiger top (10 mL each) • 1 plasma preparation tube (PPT) or lavender top EDTA (7 mL) • OMT • 2 Orasure OMT • Devices • Rapid OMT and fingerstick for all cases and controls
Labels • Serum, plasma, OMT • Subject ID label • Gender and CDC lab project number label • Mp225 • Fp225 • Seal lid with adhesive tape: must be watertight • Wrap each vial/tube in foam envelope • Devices • Subject ID label • Place each OMT device in plastic ‘BIOHAZARD’ bag
Packaging Specimens • Plastic or metal containers • Follow all instructions included • Label container with name, address and phone number of shipper • Pad between vials with absorbent wrapping material • DO NOT place ice in this container
Specimen Submission Form • Appendix E in protocol • One copy between container and shipping box • Fax second copy to: • Dollene Hemmerlein (770) 339-5915 • Krishna Jafa (404) 639-8640
Outer packaging • Bio-transporter box • Follow all instructions included • Place copy of specimen submission form between container and box (fax second copy)
Label the Shipment • ALL labels on same side, alongside each other, clearly visible • Name, address and phone number of shipper • Diagnostic specimen UN 3373 label • Orientation label (which side is ‘Up’) • Address label: name, complete facility name, shipping address, phone number • Label with ‘Person Responsible for Shipment’ and 24 h/7 d phone number (no pagers)
Shipping Options • Preferred: • Same day, on ice • Serum: centrifuge, transfer into cryotubes • Plasma: centrifuge, transfer into cryotubes, DO NOT freeze • OMT • If centrifuge not available • Same day, on ice • Serum (in red top tube) • Plasma (in lavender top tube), DO NOT freeze • OMT • Ship all rapid test devices with specimens
Shipping • Fedex with CDC account number • Typed or computer generated • Sign form • Monday through Thursday • DO NOT ship on Friday Ms. Dollene Hemmerlein/Project 225 CDC Serum Bank 602 Webb Gin House Rd. Lawrenceville, Georgia 30045 Telephone: (770) 339-5917
Supplies From CDC • Shipping containers and boxes • Labels: • Fedex • Gender, project number (e.g. Mp225) • If required: • Cold packs • Tubes and vials
Summary • Perform fingerstick and OMT rapid tests • Recruit case and 3 consecutive controls • Administer questionnaire • Ship specimens and devices
Division of HIV/AIDS Prevention, CDC Atlanta,GA Pragna Patel Patrick Sullivan Bernard Branson Kevin Delaney Duncan Mackellar Steven Ethridge Jeffrey Wiener Amy Drake Glenn Nakamura Tricia Hall Minnesota Department of Health Minneapolis, MN Stephen Swanson Tracy Sides Peter Carr Hennepin County Health Dept. Minneapolis, MN Deborah Persell Margaret Simpson New Jersey Department of Health and Senior Services Trenton, NJ Sindy M. Paul Rose Marie Martin Ken Earley Phil Brucolari Maureen Wolski Lorhetta Nichol Ayemaung Maung Rhonda Williams UMDNJ Robert Wood Johnson Medical School Eugene G. Martin Evan Cadoff Wisconsin Division of Public Health Madison, WI Alexandra Newman Jim Vergeront Kathleen Krchnavek Matt Maxwell Amy Doczy Mary Jo Hussey Acknowledgments