Download
1 / 1
10 likes | 170 Views
HYPERHOMOCYSTEINEMIA, A RISK FACTOR INTERACTING IN MODERATE AND SEVER HYPOTHYROIDISM. Mariana Purice , I.H. Ursu, A. Goldstein National Institute of Endocrinology “C.I. Parhon”, Bucharest, Romania. ABSTRACT. INTRODUCTION.

E N D
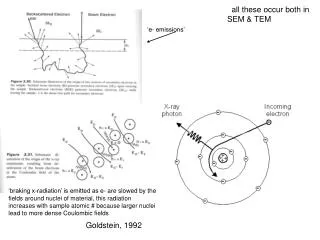
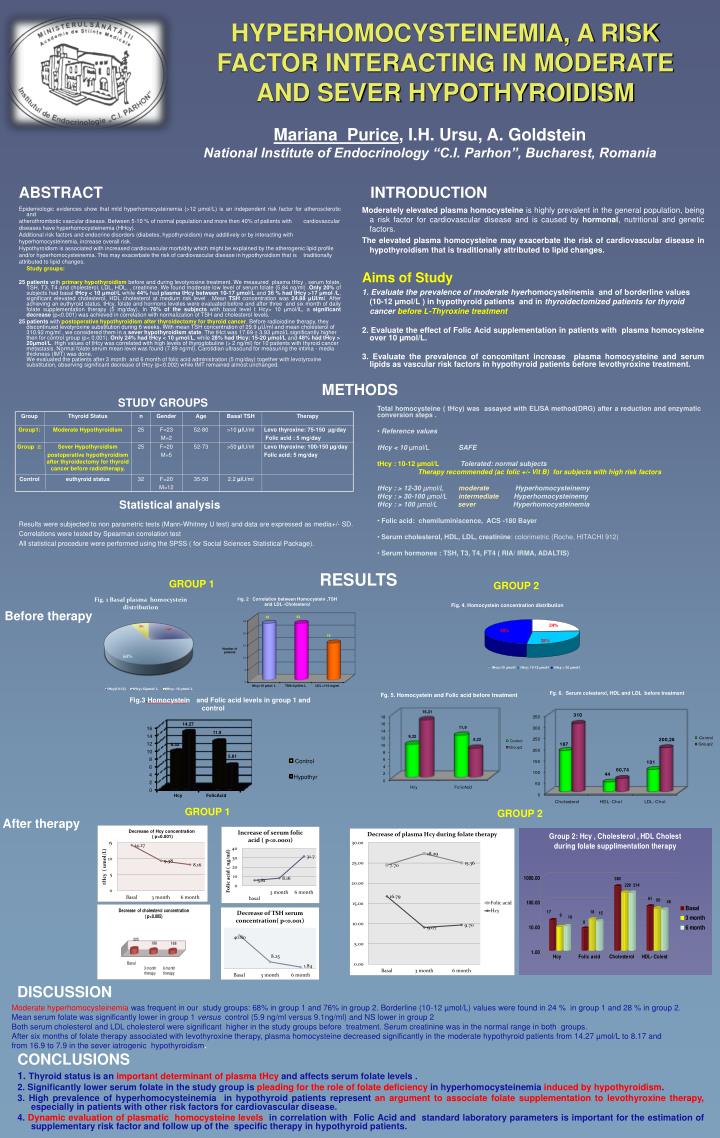
HYPERHOMOCYSTEINEMIA, A RISK FACTOR INTERACTING IN MODERATE AND SEVER HYPOTHYROIDISM Mariana Purice, I.H. Ursu, A. Goldstein National Institute of Endocrinology “C.I. Parhon”, Bucharest, Romania ABSTRACT INTRODUCTION Moderately elevated plasma homocysteine is highly prevalent in the general population, being a risk factor for cardiovascular disease and is caused by hormonal, nutritional and genetic factors. The elevated plasma homocysteinemay exacerbate the risk of cardiovascular disease in hypothyroidism that is traditionally attributed to lipid changes. Aims of Study 1. Evaluate the prevalence of moderate hyerhomocysteinemia and of borderline values (10-12 µmol/L ) in hypothyroid patients and in thyroidectomized patients for thyroid cancerbefore L-Thyroxine treatment 2. Evaluate the effect of Folic Acid supplementation in patients with plasma homocysteine over 10 µmol/L. 3. Evaluate the prevalence of concomitant increase plasma homocysteine and serum lipids as vascular risk factors in hypothyroid patients before levothyroxine treatment. Epidemiologic evidences show that mild hyperhomocysteinemia (>12 μmol/L) is an independent risk factor for atherosclerotic and atherothrombotic vascular disease. Between 5-10 % of normal population and more then 40% of patients with cardiovascular diseases have hyperhomocysteinemia (HHcy). Additional risk factors and endocrine disorders (diabetes, hypothyroidism) may additively or by interacting with hyperhomocysteinemia, increase overall risk. Hypothyroidism is associated with increased cardiovascular morbidity which might be explained by the atherogenic lipid profile and/or hyperhomocysteinemia. This may exacerbate the risk of cardiovascular disease in hypothyroidism that is traditionally attributed to lipid changes. Study groups: 25 patients with primary hypothyroidismbefore and during levotyroxine treatment. We measured plasma tHcy , serum folate, TSH, T3, T4 and cholesterol, LDL, HDL, , creatinine. We found moderate low level of serum folate (5.84 ng/ml) .Only 20% of subjects had basal tHcy < 10 μmol/L while 44% had plasma tHcy between 10-17 μmol/L and 36 % had tHcy >17 μmol /L, significant elevated cholesterol, HDL cholesterol at medium risk level . Mean TSH concentration was 24.88 μUI/ml. After achieving an euthyroid status, tHcy, folate and hormons leveles were evaluated before and after three and six month of daily folate supplementation therapy (5 mg/day). In 76% of the subjects with basal level t Hcy> 10 μmol/lL, a significant decrease (p<0.001) was achieved in correlation with normalization of TSH and cholesterol levels. 25 patients with postoperative hypothyroidism after thyroidectomy for thyroid cancer. Before radioiodine therapy, they discontinued levotyroxine substitution during 6 weeks. With mean TSH concentration of 29.9 μU/ml and mean cholesterol of 310.92 mg/ml , we considered them in a sever hypothyroidism state. The tHct was 17.69 ± 3.93 μmol/L significantly higher then for control group (p< 0.001). Only 24% had tHcy < 10 μmol/L, while 28% had tHcy: 15-20 μmol/L and 48% had tHcy > 20μmol/L. High values of tHcy was correlated with high levels of thyroglobuline (> 2 ng/ml) for 10 patients with thyroid cancer metastasis. Normal folate serum mean level was found (7.89 ng/ml). Carotidian ultrasound for measuring the intima - media thickness (IMT) was done.We evaluated the patients after 3 month and 6 month of folic acid administration (5 mg/day) together with levotyroxine substitution, observing significant decrease of tHcy (p<0.002) while IMT remained almost unchanged. METHODS STUDY GROUPS • Total homocysteine ( tHcy) was assayed with ELISA method(DRG) after a reduction and enzymatic conversion steps . • Reference values • tHcy < 10 µmol/L SAFE • tHcy : 10-12 µmol/L Tolerated: normal subjects • Therapy recommended (ac folic +/- Vit B) for subjects with high risk factors • tHcy : > 12-30 µmol/L moderateHyperhomocysteinemy • tHcy : > 30-100 µmol/L intermediateHyperhomocysteinemy • tHcy : > 100 µmol/L severHyperhomocysteinemia • Folicacid: chemiluminiscence, ACS -180 Bayer • Serumcholesterol, HDL, LDL, creatinine: colorimetric (Roche, HITACHI 912) • Serum hormones : TSH, T3, T4, FT4 ( RIA/ IRMA, ADALTIS) Group Thyroid Status n Gender Age Basal TSH Therapy Group1: Moderate Hypothyroidism 25 F=23 M=2 52-80 >10 µIU/ml Levo thyroxine: 75-150 µg/day Folic acid : 5 mg/day Group 2: Sever Hypothyroidism postoperative hypothyroidism after thyroidectomy for thyroid cancer before radiotherapy. 25 F=20 M=5 52-73 >50 µIU/ml Levo thyroxine:100-150 µg/day Folic acid: 5 mg/day Control euthyroid status 32 F=20 M=12 35-50 2.2 µIU/ml Statistical analysis Results were subjected to non parametric tests (Mann-Whitney U test) and data are expressed as media+/- SD. Correlations were tested by Spearman correlation test All statistical procedure were performed using the SPSS ( for Social Sciences Statistical Package). RESULTS GROUP 1 GROUP 2 Fig. 4. Homocystein concentration distribution Before therapy 24% 48% 28% tHcy<10 mol/l tHcy: 10-12 mol/l tHcy > 20 mol/l Fg. 6. Serum colesterol, HDL and LDL before treatment Fg. 5.Homocystein and Folic acid before treatment Fig.3. Homocystein and Folic acid levels in group 1 and control 14.27 16 11.9 14 12 9.32 10 5.81 8 Control 6 4 Hypothyr 2 0 Hcy FolicAcid After therapy DISCUSSION Moderate hyperhomocysteinemiawas frequent in our study groups: 68% in group 1 and 76% in group 2. Borderline (10-12 µmol/L) values were found in 24 % in group 1 and 28 % in group 2. Mean serum folate was significantly lower in group 1 versus control (5.9 ng/ml versus 9.1ng/ml) and NS lower in group 2 Both serum cholesterol and LDL cholesterol were significant higher in the study groups before treatment. Serum creatinine was in the normal range in both groups. After six months of folate therapy associated with levothyroxine therapy, plasma homocysteine decreased significantly in the moderate hypothyroid patients from 14.27 µmol/L to 8.17 and from 16.9 to 7.9 in the sever iatrogenic hypothyroidism. CONCLUSIONS 1.Thyroid status is an important determinant of plasma tHcy and affects serum folate levels . 2. Significantly lower serum folate in the study group is pleading for the role of folate deficiency in hyperhomocysteinemia induced by hypothyroidism. 3. High prevalence of hyperhomocysteinemia in hypothyroid patients represent an argument to associate folate supplementation to levothyroxine therapy, especially in patients with other risk factors for cardiovascular disease. 4. Dynamic evaluation of plasmatic homocysteine levels in correlation with Folic Acid and standard laboratory parameters is important for the estimation of supplementary risk factor and follow up of the specific therapy in hypothyroid patients. GROUP 1 GROUP 2