Download
1 / 57
670 likes | 1.4k Views
Biliary Conditions. NUR-224. OBJECTIVES. Discus management of patient with cholelithiasis. Use the nursing process a framework for care of –patients with cholelithiasis and undergoing laparoscopic or open cholecystectomy. Differentiate between acute and chronic pancreatitis.

E N D
Biliary Conditions NUR-224
OBJECTIVES • Discus management of patient with cholelithiasis. • Use the nursing process a framework for care of –patients with cholelithiasis and undergoing laparoscopic or open cholecystectomy. • Differentiate between acute and chronic pancreatitis. • Describe the nursing management of patients with acute pancreatitis.
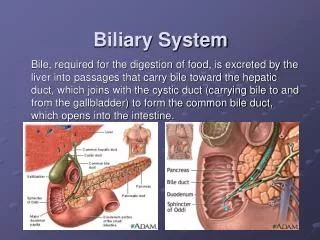
GALLBLADDER • Pear shaped organ • Stores 30-50 mL of bile • Collects, concentrates and stores bile until needed for digestion. • Releases bile into the duodenum via the common bile duct when fat is present.
BILIARY CONDITIONS • Extremely common • Interfere with the normal drainage of bile into the duodenum • 2 common problems: a. Cholecystitis b. Cholelithiasis • Common in Caucasians/Native Americans
Risk Factors • Sedentary lifestyle • Obesity • Multiparous women
CHOLECYSTITIS • Acute inflammation of the gallbladder • May result from stones may obstructing the outflow of bile • S/S pain in the ® upper abdomen that may radiate to the ® shoulder, tenderness, rigidity ® upper abdomen
CHOLECYSTITIS Acalculous Acalculous • Gallbladder inflammation without gallstones/absence of obstruction • Occurs after major surgical procedures, severe trauma & extensive burns
CHOLECYSTITIS Calculous • Gallbladder inflammation & stones that obstruct bile flow • Occurs in 90% of the clients
CHOLELITHIASIS Calculi/gallstones— • form from the solid constituents of bile • vary greatly in size, shape & composition • increasing prevalent after 40 yrs. of age; esp. women
PATHOPHYSIOLOGY • Two major types of gallstones: Pigment Stones Cholesterol Stones
CHOLESTEROL STONES • Account for 80% of gallbladder disease . • There is a decrease in bile salts & an increase in cholesterol. • Cholesterol saturated bile causes gallstones. • This acts as an irritant that produces inflammatory changes in the gallbladder.
CHOLESTEROL STONES • Are 2-3x more common in women. • Incidence increaseswith clients with diabetes. • Stones are usually smooth & are whitish yellow to tan in color.
PAIN/BILIARY COLIC • Classic symptom • Spasms occur in order to move the stone through the duct. • Excruciating ® upper abdominal pain • May occur 3-6 hours after a heavy meal • May require analgesics meperidine
JAUNDICE • Appears when the Common Bile Duct (CBD) obstruction is present. • Bile is no longer carried to the duodenum– absorbed in the blood. • Pruritus • Concentration of bilirubin > 2.5
VITAMIN DEFICIENCY • Obstruction of bile flow interferes with absorption of fat soluble vitamins intestines. • Vitamin A, D, E, K, deficiencies may be seen.
CHANGES in URINE & STOOL COLOR • Urine takes on a very dark color. • Stool no longer with bile pigments
DIAGNOSTIC FINDINGS • Abdominal x-ray • Ultrasonography • Endoscopic Retrograde Cholangiopancreatography – ERCP * nursing implications
ERCP • Flexible fiberoptic endoscope that allows for visualization of the hepatobiliary system/place stents. • 90% of the clients do well with this procedure. • The stone may be extracted or left in the duodenum to pass naturally.
MEDICAL MANAGEMENT Major Objective: • Reduce the episode of gallbladder pain & inflammation by supportive & dietary management. • Remove the cause of cholecystitis by pharmacological therapy, endoscopic procedures or surgical interventions.
NUTRITIONAL & SUPPORTIVE THERAPY • Low- fat diet • Foods to avoid • Remind client that fatty foods may bring on an episode of cholecystitis.
PHARMACOLOGIC THERAPY • Cholestyramine (Questran) • Urosdeoxycholic acid (Actigall) & Chenodiol (Chenix) are medications used to dissolve small gallstones/composed of primarily cholesterol . • 6-12 months of therapy is required to dissolve stones. • Indicated for clients who refuse surgery/surgery is to risky.
NONSURGICAL REMOVAL of GALLSTONES Extracorporal Shock Wave Lithotripsy • Noninvasive procedure • Uses repeated shock waves to disintegrate gallstones. • Requires no incision & no hospitalization. • Has been replaced – Laproscopic Cholecystectomy
SURGICAL MANAGEMENT Done to: • Relieve persistent symptoms • Remove the cause of the biliary colic • Treat acute cholecystitis
LAPROSCOPIC CHOLECYSTECTOMY • Standard of care for Rx. of gallstones. • Small incision is made through the abdominal wall at the umbilicus. • 4 small incisions are made through the abd. wall to introduce other surgical instruments. • Abdomen is insufflated with carbon dioxide – assists in visualizing abd. structures.
LAPROSCOPIC CHOLECYSTECTOMY Advantages : • Short hospital stay • Less invasive /shorter healing time • Less post-op pain/less opiod use • Early ambulation • Able to resume full activity in about 3-4 days. • Incision care is minimal
CHOLECYSTECTOMY • Gallbladder is removed through abdominal incision. • Drain may be placed – near the gall bladder bed & brought out through a puncture site for drainage. • Drain usually kept in placed for 24 hrs. then removed.
Post-op Nursing Interventions: Relieve the pain Improve the respiratory status Improve the nutritional status Skin integrity/drainage CHOLECYSTECTOMY
NURSING INTERVENTION • Fowler’s position • May have NGT • NPO until bowel sounds return, then a soft, low-fat, low-carbohydrate, high protein diet postoperatively • Care of biliary drainage system • Administer analgesics as ordered and medicate to promote/permit ambulation and activities, including deep breathing • Turn, and encourage coughing and deep breathing, splinting to reduce pain • Ambulation
Patient Teaching • Medications • Diet: at discharge, maintain a nutritious diet and avoid excess fat. Fat restriction is usually lifted in 4–6 weeks. • Instruct in wound care, dressing changes, care of T-tube • Instruct patient and family to report signs of gastrointestinal complications, changes in color of stool or urine, fever, unrelieved or increased pain, nausea, vomiting, and redness/edema/signs of infection at incision site
PANCREAS • Located in upper abdomen Functions • Exocrine function • Secrete digestive enzymes into the GI tract through the pancreatic duct. • Amylase, trypsin, lipase • Endocrine function • secretes insulin, glucagon, and somatostatin directly into the blood stream
Pancreatitis • Characterized by the release of pancreatic enzymes into the tissue of the pancreas itself hemorrhage and necrosis • Can be acute or chronic • Hospitalizations for acute pancreatitis have increase over the last 15 years • Alcoholism and gall stones are the primary risk factors.
Acute Pancreatitis • The pancreatic duct becomes obstructed and enzymes back up into the duct, causing auto digestion and inflammation of the pancreas. • Minimal organ dysfunction is present. • Characterized by edema and inflammation which is confined to the pancreas. • Affects all ages – common in middle-aged men/women • 3x higher in Afro-Americans than Caucasians
Risk Factors • Gallstones – leading cause • Alcoholism • Trauma • Infection -- viral
Acute Pancreatitis • Self- digestion of the pancreas by its own enzymes especially trypsin. • This causes injury to the pancreatic cells or activation of the pancreatic enzymes in the pancreas rather than the intestines. • Activated trypsin is in the pancreas. This enzyme can digest the pancreas and can activate other proteolytic enzymes.
Acute Pancreatitis Clinical Manifestations • Abdominal pain • Pain not relieved not by vomiting • Abdominal tenderness with muscle guarding • Bowel sounds may be absent/diminished • Hypotension, fever, jaundice
Acute Pancreatitis Assessment/Diagnostic Findings • Serum amylase and lipase levels increased • Other findings – increase in liver enzymes, bilirubin, triglycerides . • X-rays of the chest and abdomen • Abdominal ultrasound
Acute Pancreatitis Nursing management Relieve pain and discomfort • Parenteral opioids • Nonpharmacologic interventions • Bedrest • Frequent oral care • NGT suction • Clouded sensorium
Acute PancreatitisNursing management Improve breathing patterns • Semi-Fowler’s position • Change in position • Monitor pulse oximetry • C,DB/Incentive Spirometry
Acute PancreatitisNursing Management Improve nutritional status • Oral food/fluid intake in not permitted. • Monitor lab results/daily weights • Avoid heavy meals/alcoholic beverages • Diet – high CHO, low fats, low proteins.