Download

1 / 27
270 likes | 276 Views
Michigan’s Integrated Care for Dual Eligibles Proposal. Alison Hirschel Michigan Poverty Law Program July, 2012. The Timeline. Michigan awarded a contract from Center for Medicare and Medicaid Services (CMS) to design a demonstration proposal in 2011.

E N D
Michigan’s Integrated Care for Dual Eligibles Proposal Alison Hirschel Michigan Poverty Law Program July, 2012
The Timeline • Michigan awarded a contract from Center for Medicare and Medicaid Services (CMS) to design a demonstration proposal in 2011. • On March 5, 2012, Department of Community Health (DCH) released a draft proposal for comment. • On April 26, 2012, DCH submitted a substantially similar proposal to CMS • The federal comment period ended May 30, 2012. • Year long implementation proposed to begin in July, 2013.
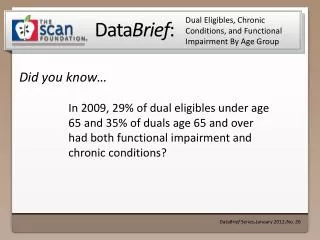
The Basics • When (and if) fully implemented, the state estimates the three year demonstration will serve 200,000 people eligible for both Medicare and Medicaid. • Current state and federal annual expenditures through Medicare and Medicaid for this population exceed $8 billion.
The Goal • “To offer high quality, seamless and cost effective care through coordinated, person-centered services that meet the unique needs of all MMEs [individuals eligible for both Medicare and Medicaid].” Proposal to CMS, p. 1
More MI goals and principles • Improved health outcomes • Improved cost-effectiveness • Extensive, on-going stakeholder process • Maintain elements of current system that are effective • Preference for community based care • Choice, autonomy, self-determination • Service integration that benefits consumers • Seamless transition from current system • Streamline administrative processes
Bifurcated System of Managed Care Entities • Separate contracts for Integrated Care Organizations (ICOs) and Prepaid Inpatient Health Plans (PIHPs). • ICOs to cover physical health and ltss • PIHPs to cover behavioral health (People with intell..developmental disabilities, serious mental illness, substance use issues). • Connection between ICOs and PIHPs through an ill-defined “care bridge.”
More basics about the proposal • Passive enrollment • Phased-in implementation: new region each quarter &, within each region, phase in by population • Risk based capitation rates with partial risk for management entities • Initial screen followed by more in-depth assessment
Services covered • “All Medicare and Medicaid services and benefits” including: • Inpatient and outpatient acute care • Skilled and custodial nursing facility care • Behavioral health services • Hospice • Home health • Community based ltc • DME • Prescription drugs
What we like: • Decent, multi-stage stakeholder process; (better opportunities for in-put than real engagement); • Focus on choice, care coordination, person-centered supports and services & self-direction (at least in theory) • Slower, staggered implementation • Balancing innovation and continuity
More we like… • Preference for community based ltc • Comprehensive set of services • ICOs and PIHPs to include consumers on governance boards • Asserted commitment to cultural competency • Not a singular focus on cost-saving
Overarching concerns • Proposal is vague in every respect, means of achieving goals not specified • Central concept of care bridge needs further development • Passive enrollment and lock-in • Insufficient track record among managed care plans in ltss
More overarching concerns • Lack of clarity re provider networks and out-of-network provider agreements • Unclear role/experience/expectations for supports coordinator/care manager • Unclear how Home Help will work • Unclear interaction w/ current waivers
More general concerns • Does state have capacity to pull this off? • How will plan work for people with special challenges such as dementia? • How much will current, positive relationships with providers be disrupted? • What happens to people who are not eligible (not dually eligible, spend-down population) or opt out? (We could go on….)
Specific issues: On-going Stakeholder Engagement (proposal, p. 22) • Promised opportunities for comments and feedback throughout implementation and operation. • Involvement of Medicare-Medicaid Eligibles (MMEs) on governance boards • Est. on-going quality focused advisory council and stakeholder group • Utilize existing entities such as Olmstead, MCAC, SLTCOP, etc.
Specific concerns: Stakeholder involvement • State needs to establish workgroups or other forums for immediate and sustained stakeholder engagement in developing Request For Proposals, fleshing out proposal, focusing on key issues, etc. • Episodic, informal, or limited stakeholder in-put no substitute for sustained and focused engagement
Specific issues: Enrollment (proposal, p. 30) • The proposal: • Passive enrollment, can opt out • 2 month open enrollment prior to implementation; 1 month to process app. • Info mailed to MMEs; toll-free number or face-to-face opportunity to speak to counselor (MMAP, enrollment broker, website) • Auto-assignment if no plan picked • Lock-in “up to” 3 mos. after enrollment until next annual open enrollment
Enrollment concerns • Passive enrollment, lock-in • Need “Choice brokers” as opposed to “Enrollment brokers” • Need community based orgs involved to help MMEs navigate • Timelines unrealistic • Insufficient info on how seamless transition will be accomplished, current services continued during transition
Specific issue: Provider networks (proposal, p. 16) • Management entities required to demonstrate adequate provider networks and core competencies • Entities required to reach out to current providers and establish linkage w/ community based delivery systems • Mechanism for out of network relationships
Provider network concerns • How much choice will MMEs have? • What does “adequate” provider network mean? Will providers have necessary core competencies, expertise & experience; accept new patients; be geographically accessible; etc. • How will out of network services be accessed and reimbursed?
Specific Issue: Care/Supports Coordination (proposal, p. 13) • Brief screen and then assignment to ICO or PIHP depending on primary needs • Use of core assessment tool with subsections tailored to individual issues • Select care/supports coordinator to lead multidisciplinary group of providers • Care bridge and Person Centered Medical Home
Specific concerns: Care/supports coordination • Confusion how the care bridge work across the ICO/PIHP divide? • Need to clarify terms • Is the MME able to choose whether the main care coordinator is from the ICO or PIHP? • What training, expertise, and availability will coordinators have? Is this role a full-time job or added on to existing responsibilities? What is the role? What about existing supports coordinators? • Is coordination/support available 24/7? Does coordinator anticipate needs or just respond?
Specific Concern: Long Term Supports and Services • Little mention of ltss specifically (limited disc. of financing, p. 5) • Managed care entities have little experience with ltc • No clarity how goal of increased community based care will be achieved • No discussion of how supports coordination will work in nh setting, how much choice of nh providers, etc. • Uncertainty re impact on waiver program both for MMEs and for those who are not MMEs.
Specific issue: enrollee protections (proposal, p. 21) • State offers 4 prong plan: • Education and outreach • Choice of providers • Appeals systems protections • Other protections quality committee, consumers on governing boards, and, possibly, creation of an ombudsman
Specific concerns: enrollee protections • Americans with Disabilities Act (ADA) compliance not specifically required • Will all communications be tested and translated into multiple languages and formats for people with special needs? Will costs of accommodations be factored into reimbursement? • Need user friendly appeal process • Will department monitor protections, enforce requirements, and implement decisions?
Specific concern: financing & reimbursement (proposal, p. 22) • Insufficient data available to DCH as proposal was being developed • Little specificity in proposal • Advocates have less expertise in this arena and are not consulted on these issues despite impact on beneficiary experience in Integrated Care for Dual Eligibles (ICDE).
Conclusion • State acknowledges vagueness regarding both key broad concepts and specific issues • Advocates have submitted pages and pages of comments and concerns. • Massive undertaking; less than 1 year until implementation scheduled to begin. • Consumer engagement required ASAP to focus planning on likely consumer challenges and experience and to assure continued adjustments during and after implementation.
Thank you! Alison Hirschel Michigan Poverty Law Program 517-394-2985 hirschel@lsscm.org