Download
1 / 30
310 likes | 517 Views
FEVER AND NEUTROPENIA. AZIZA SHAD, MD LOMBARDI CANCER CENTER GEORGETOWN UNIVERSITY HOSPITAL. INTRODUCTION. Febrile neutropenia and infections are expected treatment-related sequelae in childhood cancer Increased use of dose-intensive combinations of chemotherapeutic agents

E N D
FEVER AND NEUTROPENIA AZIZA SHAD, MD LOMBARDI CANCER CENTER GEORGETOWN UNIVERSITY HOSPITAL
INTRODUCTION • Febrile neutropenia and infections are expected treatment-related sequelae in childhood cancer • Increased use of dose-intensive combinations of chemotherapeutic agents • Fewer dosage modifications are being made for myelosuppression
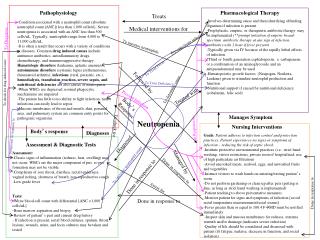
DEFINITIONS Fever • Single oral temperature of > 38.30C (1010F) or • A temperature of 38.00C (100.40F) for > 1 hour Neutropenia • A neutrophil count of < 500 cells/cumm3 or • A count of < 1000 cells/cumm3 with a predicted decrease to <500 cells/cumm3
FACTORS CONTRIBUTING TO THE RISK OF INFECTION • Degree and duration of neutropenia • Single, most important risk factor associated with infection • ANC < 1000/mm3, risk with an ANC <100/mm3, • Protracted neutropenia • ANC < 500/mm3 for more than 10 days – risk • At least 50% of febrile neutropenic patients will have an established or occult infection • 20% patients with ANC < 100/cumm3 have bacteremia at presentation
FACTORS CONTRIBUTING TO THE RISK OF INFECTION • Abnormalities in mucosal and integumentary physical defense barriers • Chemotherapy and radiation therapy • Implanted intravascular devices • Altered nutrition • Decrease in phagocyte number and function • Alteration in cellular and humoral immunity • Alteration in the endogenous microbial flora • colonization with aerobic gm –ive bacteria and fungi • Hospitalization
EVALUATION OF THE NEUTROPENIC PATIENT • Signs and symptoms of inflammation may be minimal or absent • Sites that deserve attention during the physical exam • Oral cavity and pharynx • Lungs • Perineum, including the anus • Fundi • Skin, including the bone marrow aspiration sites, central line exit site and tissue around the nails
EVALUATION OF THE NEUTROPENIC PATIENT • Laboratory tests • CBC and complete chemistry panels • At least 1 set of blood cultures from the central line and / or peripheral vein • Urine analysis • Chest X-Ray? • Respiratory signs / symptoms • If out-patient management is being planned • Gram stain and cultures of catheter exit site, urine, stool, CSF, skin biopsy, radiological studies as dictated by signs / symptoms
EVALUATION OF THE NEUTROPENIC PATIENT • Routine cultures from anterior nares, oropharynx, urine and rectum are not useful in the absence of a disease process • Infection control purposes • Nasal cultures: methicillin resistant Staph Aureus, penicillin resistant Pneumococcus, Aspergillus • Rectal cultures: Pseudomonas aeruginosa, multi-drug resistant gm-ive bacilli, VRE • Candida tropicalis in surveillance cultures has been associated with an risk for subsequent infection
WHO QUALIFIES FOR INITIAL EMPERICAL ANTIBIOTIC THERAPY? • All neutropenic patients at the onset of fever • Afebrile, neutropenic patients with signs / symptoms compatible with infection
Treatment Guidelines For Fever and Neutropenia • 2002 Guidelines for the use of Antimicrobial Agents in Neutropenic Patients with Cancer • Infectious Diseases Society of America • Antimicrobial Therapy of Unexplained Fever in Neutropenic Patients • 2003 Guidelines of the Infectious Diseases Working Party of the German Society of Hematology Oncology, German Cancer Society
Treatment Guidelines For Fever and Neutropenia These are only General guidelines • Variation in individual patients and types of infections • Settings in which patients are being treated • Anti-microbial susceptibility patterns • Underlying causes of neutropenia • No specific combination of drugs or period of treatment can be applied universally to all febrile neutropenic patients
CHOOSING THE INITIAL ANTIBIOTIC THERAPY • Consider the type, frequency and antibiotic susceptibility of bacterial isolates recovered from other patients at the same hospital • Drug allergy, hepatic or renal dysfunction may limit the use of certain antibiotics • Cisplatin, amphotericin B, cyclosporine, vancomycin and aminoglycosides should be avoided in combination, if possible, because of additive renal toxicity • Monitor drug plasma levels wherever possible
COMMON BACTERIAL CAUSES OF FEBRILE EPISODES • Gram-positive bacteria - 60-70% of positive cultures • Incidence of gram-negative infections is in some centers • Common gram-positive bacteria • Fulminant infections: Staph aureus, strep viridans, pneumococci • Indolent infections: coagulase neg staph,VRE, corynebacterium jeikeium • Common gram-negative bacteria • P. aeruginosa, E. coli, Klebsiella species • Fungal infections usually super infections • Candida species may cause primary infections
ALGORITHM FOR INITIAL MANAGEMENT OF FEBRILE NEUTROPENIC PATIENTS
2003 Guidelines of the AGIHO of the German Society of Hematology Oncology • 3 risk groups based on duration of neutropenia • Low risk: < 5 days • Intermediate risk: 6-9 days • High risk: > 10 days
2003 Guidelines of the AGIHO of the German Society of Hematology Oncology • Low Risk group • Empirical mono or duo therapy IV • Oral therapy with cipro, levo or ofloxacin + Amoxicillin/clavulinic acid • Intermediate Risk and High Risk group • Empirical mono or duo therapy IV
TREATMENT WITH INTRAVENOUS ANTIBIOTICS - MONOTHERAPY • No difference between monotherapy and multi-drug combinations for uncomplicated F&N • 3rd or 4th generation cephalosporin, piperacillin - tazobactam or carbapenem – all effective • Extended spectrum and type 1 -lactamases have reduced the utility of ceftazidime • Cefepime, imipenem and meropenem - excellent activity against strep viridans and pneumococcus • Vancomycin less frequently required with cefepime monotherapy
INTRAVENOUS ANTIBIOTICS- 2 DRUG THERAPY WITHOUT VANCOMYCIN Different 2 drug combinations have similar results Advantages Potential synergistic effects against some gram-negative bacilli Minimal emergence of drug resistant strains during treatment Disadvantages Lack of activity against gram-positives Nephrotoxicity, hypokalemia, ototoxicity Single daily dose aminoglycoside with ceftrioxone as effective as monotherapy
CEFEPIME VS CEFTAZIDIME + AMIKACIN FOR FEVER AND NEUTROPENIA • Prospective randomized trial in children • 50 febrile neutropenic episodes • Results • Both equally effective regimens • Vancomycin and antifungal agents added more frequently to ceftazidime arm • Duration of fever, hospitalization, and length of antibiotic coverage longer in ceftazidime arm • Cefepime as first choice? • Shorter duration of fever, shorter hospital stay, lower treatment cost
VANCOMYCIN PLUS MONOTHERAPY OR DUO THERAPY • Vancomycin use should be limited to specific indications - emergence of VRE • May be incorporated into initial therapy of high risk patients at institutions where penicillin resistant strains of strep viridans are common • Discontinue within 24-48 hours if no infection is identified
INDICATIONS FOR VANCOMYCIN USE IN INITIAL EMPIRIC THERAPY • Serious catheter-related infections (cellulitis, bacteremia) • Known colonization with penicillin or cephalosporin resistant pneumococci or methicillin resistant staph aureus • Positive blood cultures for gram-positive bacteria before final identification • Hypotension, fever > 400C or other cardiovascular impairment • Quinolone prophylaxis in afebrile neutropenic patients before onset of fever (risk for strep viridans) • Mucositis
WHY ORAL ANTIBIOTICS AS INITIAL EMPIRIC THERAPY? • Comparable outcomes in low risk patients treated with oral antibiotics compared to similar groups treated with intravenous therapy • Reduced cost • Out-patient management • Avoidance of catheter use • Decreased risk for nosocomial infection • Better quality of life for patient (2004 JCO)
CHOICE OF ORAL ANTIBIOTIC THERAPY • Oral regimens that have been thoroughly evaluated • ofloxacin, ciprofloxacin, ciprofloxacin plus amoxicillin-clavulanate • Quinolones • Not as effective as cephalosporins or carbapenems in treating gram-positive infections • May predispose to development of strep viridans sepsis
LEVEL OF RISK FOR ORAL ANTIBIOTICS AND OUTPATIENT MANAGEMENT • Oral antibiotics alone appear to be feasible in carefully selected, febrile neutropenic patients • May only be considered for patients with no signs / symptoms or focus of bacterial infection • Vigilant observation and prompt access to medical care 24 hours / day must be available • Preferably initiated in an in-patient setting after a minimum of 48 hours of IV antibiotics
ASSESSMENT OF RISK IN CHILDREN WITH FEVER AND NEUTROPENIA • A few oral empiric trials have been conducted in children • Lowest risk for severe bacterial infections • Initial AMC >100 /cumm3 at presentation • No obvious signs / symptoms of illness • Normal CXR • Meet hospital criteria for discharge • Cancer is in remission
MANAGEMENT OF ANTIBIOTIC REGIMEN DURING THE FIRST WEEK OF THERAPY
ROLE OF COLONY STIMULATING FACTORS IN FEVER AND NEUTROPENIA • Indications for use • Fever with ANC <100/mm3 • Sepsis • Invasive fungal infection • Primary prophylaxis for patients at high risk for developing fever with neutropenia based on prior treatment history • GCSF and GMCSF
DO COLONY STIMULATING FACTORS HELP IN FEBRILE NEUTROPENIA? • COG Study – April 2005 • Randomized study of antibiotics with/without GCSF in 67 patients (59 with ALL) • Results • GSCF significantly reduced duration of neutropenia (4 vs. 13 d) • Reduced days of in hospital (4 vs. 5 d) • No difference in resolution of fever, duration of IV or oral antibiotics, antifungal therapy or shock