Download
1 / 33
400 likes | 1.17k Views
Inflammatory Response: Current Concepts. Edward R. Sherwood, M.D., Ph.D. Department of Anesthesiology The University of Texas Medical Branch Shriners Hospital for Children Galveston Burns Unit Galveston, Texas. Inflammation.

E N D
Inflammatory Response: Current Concepts Edward R. Sherwood, M.D., Ph.D. Department of Anesthesiology The University of Texas Medical Branch Shriners Hospital for Children Galveston Burns Unit Galveston, Texas
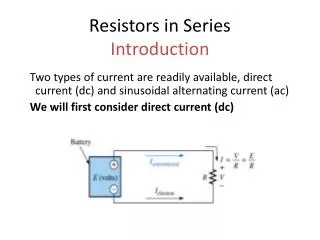
Inflammation • A protective response that removes sources of injury and facilitates tissue repair • Uncontrolled or inappropriate inflammation can cause injury • Inflammation-associated injuries during the perioperative period and the ICU • Thrombosis (myocardial infarction, stroke) • Acute lung injury, ARDS • Metabolic disturbances (hyperglycemia) • Hemodynamic dysfunction (hypotension) • End organ dysfunction (renal, hepatic insufficiency) • Pain
Classification of Inflammation • Acute inflammation • Occurs over hours, days or weeks • Characterized by vasodilation, fluid exudation and neutrophil infiltration • Caused by acute trauma, surgery, acute infection • Chronic Inflammation • Occurs over weeks, months or years • Characterized by vasodilation, fluid exudation and mononuclear cell (lymphocyte/monocyte) infiltrates. • Presence of concomitant repair (fibrosis) • Rheumatoid arthritis, atherosclerosis, inflammatory bowel disease
Acute Inflammation • Initiation • Increased vascular caliber and flow • Increased vascular permeability • fluid exudation and edema formation • Leukocyte infiltration (mainly neutrophils) • Amplification • mediated by soluble and cellular factors • Resolution • mediated by removal of source, anti-inflammatory cytokines, cholinergic nervous system and apoptosis
Initiation of Acute Inflammation • Increased Vascular Diameter and Flow • Arteriolar dilation and opening of new capillary beds • Functional importance • Delivers soluble mediators and leukocytes to site of injury • Promotes transvascular fluid flux • Clinical signs • Erythema and warmth • Pathology • Systemic vasodilation, low systemic vascular resistance, hypotension
Mediators of Increased Vascular Diameter and Flow Nitric Oxide (NO) Vasodilatory Prostaglandins
Initiation of Acute Inflammation • Transvascular Fluid Flux • Increased hydrostatic pressure causes net outflow of fluid from vascular compartment • Increased vascular permeability (to water, solute and protein) • Formation of endothelial gaps • Formation of transcytoplasmic channels • Direct or leukocyte-mediated endothelial injury • Functional importance • Delivers soluble mediators (antibodies, acute phase proteins) to site of injury • Clinical signs • Edema formation • Pathology • ARDS, interstitial edema
Burn Shock • Edema formation • Increased vascular permeability • Solutes • Electrolytes • Colloids • Decreased plasma oncotic pressure (hypoproteinemia) • Intravascular hypovolemia • Increased systemic vascular resistance • Tissue hypoperfusion, metabolic acidosis
Burn Shock: Edema Formation From Demling R, J Burn Care Rehab 26:207, 2005
Mediators of Increased Vascular Permeability • Histamine • Bradykinin • Substance P • Leukotrienes
Initiation of Acute Inflammation • Leukocyte (neutrophil) Infiltration • Process • Margination • Rolling • Adhesion • Transmigration • Chemotaxis • Functional importance • Phagocytosis, removal of bacteria and debris • Pathology • Acute lung injury, ischemia-reperfusion injury
Neutrophil Adhesion and Chemotaxis 1 Rolling 2 Adherance 3 Transmigration Lectins integrins ICAM-1 Endothelium E-selectin P-selectin PECAM 6 Apoptosis 4 Chemotaxis: Chemokines Bacterial products LTB4 5 Phagocytosis Adapted from Seely et al, Crit Care 7:291-307, 2003
Ischemia-Reperfusion Injury 2 3 4 5 6 1 Adapted from Shernan, Anesthesiology Clinics of North America 21:2003
Interactions Between Inflammation and Coagulation Endothelial Cell Macrophage/ Monocyte TNF IL-1 Activated Protein C Intrinsic Pathway (-) Tissue Factor Degradation of Va and VIIIa VIIa Tissue Factor Pathway Inhibitor (-) VIIIa IXa Xa Binds TF-VIIa Complex + Fibrin clot Va Anti-Thrombin III Macrophage/ Monocyte Activation Thrombin Binds Thrombin
Role of Complement in Systemic Inflammation Adapted from Rittirsch et al, Nat Rev Immunol 8:776, 2008
Potential Thrombotic Complications Associated with Perioperative Inflammation • Myocardial Infarction • Inflammation is associated with increased risk of plaque rupture and acute coronary syndromes • Koenig et al, Arthersler Thromb Vasc Biol 27:15, 2006 • Risk of post-operative MI associated with SNPs in IL-6, ICAM-1,CRP and E-selectin genes • Podgoreanu et al, Circulation 114:I275, 2006 • Stroke • Risk of post-operative stroke in cardiac surgery patients associated with SNPs in IL-6 and CRP genes • Grocott et al, Stroke 36:1854, 2005
Systemic Effects of Inflammation Myocardial depression Cachexia, Fever Edema Pain Erythema Edema Metabolic Dysfunction Adapted from Abbas et al, Cellular and Molecular Immunology, 2001
Sepsis and SIRS Tachycardia Tachypnea Leukocytosis or leukopenia Fever or hypothermia Severe Sepsis/SIRS Hemodynamic alterations Hypotension, decreased SVR Tissue Hypoperfusion or impaired oxygen utilization Lactic acidosis Organ Dysfunction Renal failure, mental status changes, thrombocytopenia, ARDS,coagulopathy Metabolic dysfunction Hyperglycemia The Systemic Inflammatory Response Syndrome (SIRS) and Sepsis Bone et al, Crit Care Med 20, 1992; Bone et al Chest 101, 1992 Levy et al, Crit Care Med 31, 2003
Current Treatment of Severe SIRS/Septic Shock • Cardiopulmonary/Organ-specific Support • Goal directed fluid resuscitation • Inotropic support • Mechanical ventilation • Treat metabolic, coagulation and end organ dysfunction • Remove infection/sources of inflammation • Antibiotics • Drain Abscess • Excise Necrotic/Inflamed Tissue
Potential Anti-inflammatory Treatment Approaches • Block/remove inflammatory mediators • Inhibit inflammatory response • Reduce cellular injury • Inhibit coagulation cascade
Anti-inflammatory Therapy of Sepsis:Block Mediators TNF-MAb sTNFr TNF-MAb IL-1ra IL-1ra PAFra TNF-MAb Anti-bradykinin sTNFr ibuprofen TNF-MAb PAFra 0.5 0.67 1 1.5 2 Odds ratio benefit injury Adapted from Natanson et al, Crit Care Med 1998
Anti-inflammatory Therapy of Sepsis • Hemofiltration • Complement antagonism • C1 inhibitor (blocks classical/lectin pathways) • Anti-adhesion molecule • Selectins, ICAM-1 • Blockade of Nitric Oxide • iNOS inhibition, NO scavenging • Phosphodiesterase inhibitors • Pentoxifylline, milrinone • Anti-oxidants • Selenium, N-acetylcysteine, Vit. C and E
Steroids in Septic Shock High dose (30 mg/kg prednisone) Short term (1-3 days) steroids Cronin et al, Crit Care Med 1995
Steroids in Septic Shock • Patients in septic shock with low adrenal reserve (corticotropin stimulation test) showed improved survival when treated with replacement corticosteroids • Replacement dose steroids may only have benefit in septic patients with vasopressor-refractory hypotension (CORTICUS), Z. Thomas, Ann Pharmacother 41:1456, 2007 • ‘Intravenous corticosteroids (hydrocortisone 200–300 mg/day, for seven days in three or four divided doses or by continuous infusion) are suggested in patients with septic shock whose blood pressure is poorly responsive to fluid replacement and vasopressor therapy.’ Surviving Sepsis Campaign, Crit Care Med 36:296, 2008 Annane et al, JAMA 288:862, 2002
Biology of Activated Protein C Normal Sepsis Proteolysis of factors Va and VIIIa Profibrinolysis Activated protein C Protein C Inflammation Thrombosis Consumption of Protein C inhibit Cytokine Production Fibrin clot Formation Fibrin clot Formation Cytokine Production induce Tissue factor Tissue factor Adapted from Kumar et al, Robbins Textbook of Pathology
Treatment of Severe Sepsis with Activated Protein C • Mortality due to all causes significantly improved in patients treated with activated protein C (APC) • 1 life saved for every 16 patients treated with APC • Decreased IL-6 and D Dimer levels in APC-treated patients Activated protein C 75.3% placebo 69.2% Bernard et al NEJM 2001
Treatment of Severe Sepsis with Activated Protein C From Vincent et al, Crit Care 10:R274, 2006
Treatment of Patients with Severe Sepsis and at Lower Risk of Mortality with Activated Protein C Single organ failure or Apache II score less than 25 From Abraham et al, NEJM 353:1332, 2005
Efficacy of Activated Protein C in Patients with Severe Sepsis and Elevated Troponin Levels NormalTroponin ElevatedTroponin From John et al, Int Care Med 33:212, 2007 APC suggested in adult patients with septic shock, organ failure and high risk of death without contraindications. Surviving Sepsis Campaign, Crit Care Med 36:296, 2008
The Autonomic Nervous System and Inflammation From: Czura and Tracey J Int Med 257:156, 2005; Metz and Tracey Nat Immunol 6:756, 2005 Pavlov et al Crit Care Med 35:1139, 2007
Summary • Our understanding of inflammation at the cellular and molecular levels has advanced significantly during the last 20 years • These advances have not yet translated into widespread clinical benefit in management of acute inflammatory processes although promising results with newer approaches have been obtained in some settings (e.g. Activated Protein C for severe sepsis)