Download
1 / 33
330 likes | 439 Views
MEMORY. Tim Kimbrell, M.D. OBJECTIVES. overview of memory models differences between declarative (explicit) and procedural (implicit) memory kindling/sensitization and its relationship to memory neuropsychological basis of memory and common forms of amnesia. OVERVIEW.

E N D
MEMORY Tim Kimbrell, M.D.
OBJECTIVES • overview of memory models • differences between declarative (explicit) and procedural (implicit) memory • kindling/sensitization and its relationship to memory • neuropsychological basis of memory and common forms of amnesia
OVERVIEW • Changes in neural networks must occur to encode and retrieve information • A memory is access to previously learned information (experience) • Bottom line: Brain function and ultimately Brain structure are changed with experience (learning)
MOTIVATION OR EMOTIONAL MEANING • Classic example of inverted “U” curve applies to memory/learning, cerebral blood flow, performance, etc. (Gur and Gur) • Mild to moderate attention/arousal are necessary • Basic science courses re a marathon, not a sprint • Fear of failure: desire to do your best
DECLARATIVE OR EXPLICIT MEMORY • Conscious or cognitive memory • Distinct facts and your awareness of knowing them (Arkansas won the Cotton Bowl) • All important in Medical School • Key: How long will you remember this stuff?
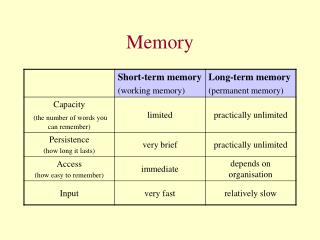
DECLARTAIVE/EXPLICIT MEMORY • SHORT-TERM: SECONDS TO MINUTES • Hear it/see it --think about it • Association cortex -- Prefrontal cortex • Working memory is an example • Ask patient to remember 3 objects
DECLARATIVE/EXPLICIT MEMORY • LONG-TERM: HOURS/DAYS TO A LIFETIME Association Cortex Medical temporal Prefrontal cortex What did you have for breakfast on Tuesday? What year were you married?
PROCEDURAL (IMPLICIT) MEMORY • Knowing how to do things without “thinking” -- swing a golf club, play piano • Storage mechanism: inherent to various sensory and motor areas • Cerebellum/amygdala known to be important
MEMORIES AND CIRCUITS • REVERBERATING MODEL: DYNAMIC IN NATURE • Stimulus enters the pathway and continues to bounce back and forth • Information “burned as a trace into the living” and thus localized • Though discredited, probable role in autobiographical memory
CONVERGENCE MODEL • Convergence of 2 excitatory signals giving change at a synaptic level (plastic) • Similar to post tetanic potentiation • Arousal is accounted for • Localization is not required • Experience changes the anatomy of the brain
APLYSIA STUDIES • Kandel demonstrated plasticity and will win the Nobel Prize • Studied a simple reflex in sea slug • Photographed morphologic change with experience/learning
HABITUATION • Repeated stimulation: attenuated/decreased response • What causes the neuron to fire? • Calcium influx decreases • If not firing, less glutamate needed, decreased mobilization and receptor number
SENSITIZATION • Restoration and potentiation of the response • Apply a noxious stimuli to sensory system • Increase neurotransmitter release • Increase “active zones” at the synapse • Inhibit protein synthesis-- block effect
PLASTICITY Sensory and motor neurons “store” information in a distributed network that is modifiable by experience and results in a change in synaptic strength
LONG TERM POTENTIATION (LTP) • Frequent stimulation/sensory input • Glutamate release and binds to NMDA receptors mediating increase in Calcium influx • Activation of phosphoproteins and transcription pathways change post synaptic structure
LONG TERM DEPRESSION/HABITUATION • Low frequency stimulation over time • Inhibition of “Meaning/significance” • Frequent half-ass attempts are not productive
ANATOMY • All brain regions play a role • Association cortex • Visual/Verbal/olfactory = sensory long term storage • Cerebellum: Procedural and declarative • Frontal cortex: Awareness/Consciousness
LIMBIC SYSTEM • Older, more primitive regions of brain • Grande Lobule Limbique • Emotional significance is contributed • Arousal “system”
LIMBIC SYTEM (continued) • Hippocampus/Amygdala; Cingulum septal region, anterior thalamus orbitofrontal cortex hypothalamus • Emotional significance provides motivation median forebrain bundle/fornix
HIPPOCAMPUS/MEDIAL TEMPORAL Most studied region related to memory • Assimilates short term to long term memory distributes to cortical regions for storage • perfused by end arteries: easily damaged • concentrated Glucocorticoid receptors
KLUVER-BUCY SYNDROME • Primates after undergoing bilateral temporal lobectomy • Hyperorality, hypersexuality and placidity • Amygdala resection necessary for full syndrome • Total amnesia: need bilateral injury to Hippocampus and possibly other medial structures
PATIENT HM • Most famous/studied patient in neurology • Bilateral hippocampal resection • Complete anterograde amnesia • Dominant Hippocampus: Auditory deficits • Non-dominant Hippocampus: Visual deficits • Cueing: make use of what you have
PRIMING • Interface between declarative and procedural • Latency between presentation and identification • HM insisted he hadn’t seen the picture • Retention of procedural memory w/o declarative
PATIENT HM (continued) • Mirror writing improved with practice • Ribot’s Law: oldest memories are most resistant to damage or decay • Natural decay: Review notes intermittently
PHARMACOLOGY • Glutamate : excitatory; make $$$ • Glycine: spinal cord excitation • GABA: inhibitory; benzodiazepine/ETOH • Acetylcholine: Displace Mg ion at NMDA receptor • Avoid anticholinergics in elderly • nucleus basalis
AMNESIA • Specific defect in declarative memory - other functions preserved • Retrograde: Loss of stored memories • Anterograde: Inability to form new memory
ALCOHOLIC BLACKOUTS • ETOH mechanism of action • Sensitization occurs • Cross reactivity with Benzodiazepines • Use long acting agents
WERNICKE-KORSAKOFF’S • Occurs with alcohol dependence • Destruction of mamillary bodies (loop of Papez) • Can be arrested if caught early
SHORT DURATION AMNESIA • Partial complex seizures: episodic • Medial temporal lobe seizure focus • Basilar artery migraines • Origin of posterior cerebral arteries
LONG DURATION AMNESIA • Herpes simplex encephalitis • Attacks medial temporal lobe (anterograde amnesia) • May resemble Kluver-Bucy
PSYCHOGENIC AMNESIA • Fugues and dissociative disorders • Stressor often involved • Most often retrograde in nature • Frequently clears with time • Retains ability to form new memories • “Knuckleheads” need best assessment
ASSESSMENT • Complete history and physical • Keep a wide differential diagnosis • Examine sensory systems • Make use of imaging/EEG