Download
1 / 43
430 likes | 583 Views
Measuring the epidemic: 2 nd Generation Surveillance and the Asia Epidemic Model (AEM). USAID SOTA meeting Washington DC Oct. 7, 2002 Stephen Mills Family Health International Asia Regional Office Bangkok, Thailand. Topics. Update on 2 nd generation surveillance in Asia

E N D
Measuring the epidemic:2nd Generation Surveillance andthe Asia Epidemic Model (AEM) USAID SOTA meetingWashington DCOct. 7, 2002 Stephen Mills Family Health International Asia Regional Office Bangkok, Thailand
Topics • Update on 2nd generation surveillance in Asia • The role of modeling: the Asia Epidemic Model (AEM) • Examples: • Cambodia – various uses • The role of IDU HIV transmission in heterosexual epidemics
Increasing scrutiny of data showing prevention intervention effects
The Good News • Number of countries with some level of quality surveillance, particularly behavioral surveillance, has increased • Our understanding and resolution of some problems in design, sampling, analysis, etc. have improved • Increasing examples where surveillance has helped to stimulate new and adjust old interventions
Examples of behavioral surveillance Place Major uses and findings • Bangladesh Risk reduction in a low prevalence setting
% of IDU reporting ever sharing equipment in the past week – Bangladesh • Overall HIV prevalence low among IDU (< 3%) • Surveillance showed decreased sharing following introduction of needle exchange program (NEP) • In Rajshahi, decreased sharing associated with NEP participation Needle exchange introduced Source: IEDCR, Gov of Bangladesh; Jenkins, Rahman, et al.
Examples of behavioral surveillance Place Major uses and findings • Bangladesh Risk reduction in a low prevalence setting • Cambodia Risk reduction linked to decreases in HIV and STIs
Condom use, HIV and STI prevalence - Brothel-based CSWs, Cambodia 1996-2001 Condom use HIV Source: NCHADS 2000-2002, Ryan et al 1998
Examples of behavioral surveillance Place Major uses and findings • Bangladesh Risk reduction in a low prevalence setting • Cambodia Risk reduction linked to decreases in HIV and STIs • Tamil Nadu, Evaluation of large India intervention program
% of truckers/helpers and factory workers reporting non-regular sex partners in the past year – Tamil Nadu, India Source: AIDS Prevention and Control Project (APAC), VHS, Chennai
% of FSWs, truckers/helpers, and factory workers reporting condom use with last non-regular sex partner – Tamil Nadu, India Source: AIDS Prevention and Control Project (APAC), VHS, Chennai
Examples of behavioral surveillance Place Major uses and findings • Bangladesh Risk reduction in a low prevalence setting • Cambodia Risk reduction linked to decreases in HIV and STIs • Tamil Nadu, Evaluation of large India intervention program • Indonesia Difficulties in changing behaviors in a low prevalence setting
% of port workers and truckers reporting two ways or more of preventing HIV infection – various sites in Indonesia Source: University of Indonesia; FHI
% of port workers and truckers reporting condom use during last sex with FSW – various sites in Indonesia Source: University of Indonesia; FHI
Examples Place What has BSS shown • Bangladesh Risk reduction in a low prevalence setting • Cambodia Risk reduction linked to decreases in HIV and STIs • Tamil Nadu, Evaluation of large India intervention program • Indonesia Difficulties in changing behaviors in low prevalence setting • Nepal Behavior change in a changing risk environment
% of transport workers and laborers reporting consistent (“Always”) use of condoms with FSWs in the past year – Terai area, Nepal Source: New Era; FHI
% of transport workers and male laborers reporting sex with a FSW in the past year – Terai area, Nepal Huge rise in number of sex establishments Source: New Era; FHI
What’s missing? • Estimates of : • HIV trends in the future based on behavioral patterns • HIV infections averted from behavior change • HIV infections from various modes of transmission and their contribution to the overall epidemic • Such estimates require modeling techniques
The Asian Epidemic Model • A model focused on replicating the dynamics of Asian epidemics • Developed by Tim Brown and Wiwat Peerapatanapokin, East-West Center • Simple model - four transmission routes: • sex work; needle sharing; intramarital & pre- & extra-marital sex; mother to child • MSM in development • Key inputs (variable by year) • sizes of important populations • behaviors over time • Key output: epidemiological trends over time
Fitting an epidemic in the AEM Transmission Behavioral trends Epidemiological trends parameters • Behavioral trends from existing data are given as inputs • Transmission parameters are then varied until trends • in HIV from the model are in reasonable agreement with • observed HIV trends • These transmission parameters include: • - probability of HIV transmission • - STD and circumcision cofactors
Key Inputs and Assumptions • Models are only as good as their inputs and assumptions • careful analysis of existing data is needed • to ensure inputs are realistic • to validate outputs • transparency is essential • Important role of 2nd generation surveillance • The model should fit the historical patterns observed in HIV infections
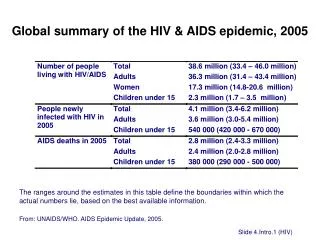
The Cambodian HIV Epidemic - a History • Highest national HIV prevalence in Asia • Epidemic initially fueled by men and commercial sex partners • Recent data however, shows prevention is having an impact, and HIV prevalence is falling in sentinel groups • HIV among direct sex workers peaked at 41% in 1996 and by 2000 had fallen to 31% • HIV has reached into the general population • Prevalence among antenatal clinic attendees peaked at 3.2% in 1997 and had declined to 2.3% by 2000 • But while the epidemic is slowing, better understanding of past and future trends is required to better direct the response
Key behavioral inputs and trends • The percentage of men having sex with sex workers has fallen • 27% in 1996 to 11% of adult males in 2000 • Condom use • Increased from 15% to 86% in brothel sites • Low between husband/wife – 0.6% • Extramarital sex - 35% (estimated) • Brothel-based sex workers have 3.2 clients/night • STDs among sex workers fell from 39% in 1996 to 23% in 2001
AEM Fit for Cambodia White lines are HIV trends from observed data Colored lines are AEM generated HIV trends Direct and indirect sex workers General population males General population females
HIV Infection in Cambodia over timeNew, cumulative and current HIV infections
Prevention efforts in Cambodia have paid huge benefits Red line represents what might have been if behaviors had not changed Infections prevented
Sustaining past successes in sex work is essential to keeping HIV under control. If condom use in direct sexwork were to fall to 60% in 2002, the epidemic would re-establish itself. Supposing condom use drops to 60% starting 2002
Changing Routes of Transmission • The Cambodian HIV epidemic is dynamic • As one route is controlled others assume importance • Dominance of sex work has now shifted to dominance of husband-to-wife infections • Over the next 3 to 4 years, mother-to-child transmission will become dominant
The routes of transmission are changing rapidly in 2002: Spousal transmission is 42% Children are now 35%The response should adapt to address these changes
Implications • Current prevention efforts must be sustained • The epidemic has changed dynamically over the last decade • New initiatives are needed to address • Husband wife infections • Continuing infections in sex work • Pediatric infections • MSM (not included in model)
Other applications of AEM • Exploring the impact of IDU and MSM sexual networks on more “generalized” transmission of HIV • Recent application looked at how many HIV infections would be averted by keeping HIV among injecting drug users at low levels • To be published in the International Journal of Drug Policy by Tobi Saidel/FHI and others
Role of IDUs in heterosexual epidemics • Parameters needed • Size of IDU population • Sexual behavior of IDU population, including commercial sex and non-regular sex partners • Time of HIV entrance into IDU population • Parameters were taken from research conducted in several settings in India
Proposed IDU Scenarios Scenario I (Early commercial sex epidemic) • High volume of commercial sex • Low prevalence among sex workers • Look at low, medium and high prevalence among IDUs Scenario II (Advanced commercial sex epidemic already underway) • Assume high prevalence among sex workers • Look at low, medium and high prevalence among IDUs Scenario III (“Controlled” commercial sex epidemic) • Assume reducing epidemic among sex workers • Look at low, medium and high prevalence among IDUs
Conclusions and policy implications of the IDU analysis • Spread of HIV among IDUs can lead to large-scale heterosexual spread • Early interventions to IDU have the greatest impact on the entire population
Asia’s unappealing population groups in need • Hard-to-reach populations or hard-to-change governments? • Population groups which are first affected and fuel the HIV epidemics of Asia continue to be “unappealing” for governments: • Injection drug users • Men who have sex with men • Migrating individuals of other nationalities or ethnic groups • Double whammy: • Lack of interventions PLUS • Lack of surveillance and monitoring which indicates an epidemic
HIV prevalence among injection drug users in Kathmandu, Nepal, 1991-2001 Percent
Looking towards the future • Most countries still do not have adequate coverage of surveillance in appropriate population groups and geographic areas • Epidemics are sometimes missed because of concentration of surveillance in donor-covered intervention areas • Support for national surveillance critical • Stimulates appropriate intervention coverage, not only by USAID but other donors as well • Feeds into modelling programs which provide estimates of impact