Download
1 / 43
430 likes | 438 Views
DRGs and per case financing. Prof Ric Marshall OAM The University of Sydney. HOSPITAL BUDGET MODELLING IN A DRG ENVIRONMENT. http://www.health.vic.gov.au/pfg/pfg2005/pfg0506.pdf. MODELLED BUDGETS EXAMPLE. Inpatient budget estimates. Inpatient budget/expenditure estimates

E N D
DRGs and per case financing Prof Ric Marshall OAM The University of Sydney.
Inpatient budget estimates • Inpatient budget/expenditure estimates • Total hosptial budget for period • Multiplied by IFRAC • HOSPITAL EXPENDITURES AND IFRACS.xlsx
The modelling process • Inpatient budgets by hospital • Inpatient volumes by DRG by hospital • Cost weights by DRG • Price from total inpatient budget • IF COSTWEIGHTS ARE REBASED • Allocate modelled budget by weighted DRGs • Adjust for redistributions above 5% • JUL AUG DRG DATA MODEL IT2.xlsx
GENERAL CHECKS/CORRECTIONS • Alignment of expenditure data and activity data • Cleaning up data by deleting test hospitals data • Aggregations of clinics to best approximate a major teaching hospital for benchmarking purposes. • Rechecking estimated IFRACS. • Rechecking grouping patterns of hospitals • Review grouper logic • Compare hospital level casemix patterns with peer hospitals • Check changes in casemix across time periods.
Specific corrections • Check for missing data Hosp A Hosp B • Check for missing expenditure data • Allocate clinics to hospitals?? Or model budgets independently?? • Check hosp X for overcounting of cases or underestimate of current revenue. • ??Duplicate data • ??Admitted outpatients • Ifrac • Check Hosp Y and Hosp Z For whereabouts of revenue and ??Cases.
Managing demand for hospital services • Demand is very elastic. • What is the right amount? • Is more better? Prevention investment? • Targets, incentives to substitution or both? • Engaging community – self care • Referral gatekeeper – copayments (equity) • Budgetary restraint a weak signal.
Target setting • Based on projection or current baseline • Same as last year’s targets • Same as last year’s actuals • Adjustment for growth • Adjustment for efficiency dividend • Planned service implementation – geographical redistribution • New services and technology allowance
Innovation, research and development • Cannot be covered by DRG weights based on previous year’s costings. • Must be covered by funding supplementation – then becomes absorbed in DRG costs. • Low volume high cost exceptional services OK for DRG funding if accurately costed • Usually high fixed costs relatively low variable.
Data sets required for DRG funding of hospital services • Activity • Data set specification • Coding rules– counting rules– admission rules • Expenditure previous years’ – quarters’ • Standard chart of account - for patient costing • Cost disaggregation standard models. • Budget and planning estimates • Price lists
REPORTING FEEDBACK • The key to • GOOD DATA • EFFICIENCY GAINS • PERFORMANCE IMPROVEMENT • The basis for rational planning • A primary mechanism to assess innovation and investment priorities.
Standard reports may include • Productivity • Complexity • Allocative efficiency • ‘doing the right things’ • Technical efficiency ‘doing things right’ • Coding Completeness • And various quality indicators • Outcome – Process • Some examples follow …
Productivity • Performance in total Weighted Episode (WEs) of all hospitals • Overall performance in total WEs against target by hospital • WEs by Major Diagnostic Categories (MDC) for Medical Diagnosis Related Group (DRGs) by hospital • WEs by MDC for Procedural DRGs by hospital • Top 10 increment DRG families by hospital • Top 10 decrement DRG families by hospital
Complexity • Casemix Index of Medical and Procedural DRGs of all hospitals • Casemix Index (CMI) by MDC by hospital • Average WEs per patient by MDC in by hospital • Average number of episodes per patient by MDC by hospital • Casemix – “1 Year On”
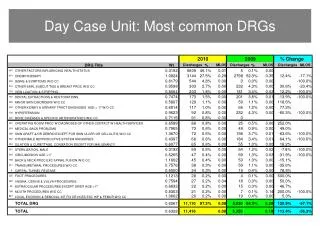
Allocative Efficiency • Percentage same day episodes by MDC of Medical and Procedural DRGs by hospital • Change in same day episodes of Ambulatory Medical DRGs • Percentage of episodes admitted via A&E Department by MDC by hospital
Technical Efficiency • Average Length of Stay (ALOS) of Medical & Procedural DRGs of all hospitals • Change in ALOS by MDC by hospital • Cost per weighted DRG by hospital
Coding Completeness • Percentage of total multi-day episodes for Medical and Procedural DRGs by severity level in all hospitals • Percentage of total multi-day episodes with Major Co-morbidities and Complication (MCC) by MDC for Medical DRGs by hospital • Percentage of total multi-day episodes with MCC by MDC for Procedural DRGs in all hospitals • Percentage of total multi-day episodes with MCC by MDC by hospital • WE / CMI by discharged specialty: 4-year trend analysis by hospital
DRGs – QUALITY AND SAFETY Terri.jackson@ualberta.ca
THE FIRST IDEA OF EFFICIENT PRICE • Data and information for fair and accurate costing and pricing (1) • What is efficient in terms of a reasonable price to pay? • what is the budget? – realistic quality? • Accuracy in costing – capital costs – sector differences – lumpy costs (eg redundancies)? • What about regional cost/salaries/inputs price variations? • Differences in packaging – eg include workup? • Scale of operation? • Equivalent developing models of care?
THE SECOND IDEA OF EFFICIENT PRICE • The Payment System – what are you actually paying for? HEALTH SYSTEM OPERATORS, REGIONS, HMOs NHIF MoH INSURERS PATIENT EMPLOYED PRACTITIONERS Drug, MD SUPPLIERS SUPPORT SERVICES MANUFACTURERS HOSPITALS, HEALTH CLINCS, PRACTITIONERS
Coding activity to DRGs • DRG grouper software online in PAS systems in hospitals • Immediate feedback on DRG effect of coding • Code finder functions for DRG • optimisation • Batch or individual record grouping • Patterns of activity by DRG • DRG pattern reporting and feedback loops
Types of Costing (1/2) • Clinical Costing • Bottom up costing approach • Each patient episode is a product • Requires data of all goods and services consumed in the treatment of individual patients • Allows analysis of resource use by individual patient episode 26
Types of Costing (2/2) • Cost Modelling • Top down approach • Relies on the use of ‘service weights’ and/or other generalised utilisation statistics 27
Why patient costing? • Patient costing provides detail at the individual patient episode • Easier to apply patient costing to other patient types • Patient costing systems are a good data repository 28
Monitor has been working on costing development for some time 29
Reference costs are not considered to be fit for purpose in the long run • Issues with Reference costs • Poor data quality and lack of credibility (e.g. 1 in 8 submissions contained materially incorrect costs, significant unexplained variations in unit costs) • Lack of clinical validity (e.g. cost relativity do not match with clinical input) • Lack of granularity • Poor input data 30
PLICS data – currently collecting to see how it can be used (1) • For participating trusts • A trust pack (high level benchmarking) • Further engagement events to help us develop future guidance and assessing the regulatory burden • We opened a pilot 2012/13 collection on 12 June 2013 and closed on 27 September • Focused on Admitted Patient Care • 66 acute trusts took part in the collection and provided data • Cost data provided are at cost pool level • Trusts also provided coding information • We also collected information to aid our understanding of trusts’ approach to costing • For Monitor • Assessing the data quality • Data exploration (e.g. PLICS vs. Ref Costs, sampling) • Benchmarking potentials • Evaluating the potential of using PLICS for pricing / currency development 31
Example of Pilot PLICS CollectionNote: This is a partial snapshot only (it is not a full data sheet) 32
PLICS are now widely implemented across the NHS, especially among acute providers 33
PLICS data – currently collecting to see how they can be used (2) • Nearly 70% of acute trusts have now implemented PLICS. Previous studies also showed that it could bring the following benefits: • Improved accuracy and consistency • Greater granularity • Greater transparency on cost drivers and what drives cost variations • Greater potential for benchmarking, currency design and pricing development 34
In Summary • Understanding the real cost of NHS services will enable the right prices to be set • Costing services accurately has the potential to deliver higher quality care to patients and better value for tax payers in the long term - through better prices and improved information for decision makers and providers • Having accurate patient level data is key to identifying the drivers of costs - and also the potential opportunities for improved quality of service for patients through innovation 35
Australia National hospital cost data collection NATIONAL HOSPITAL COST DATA COLLECTION COST WEIGHTS FOR AR-DRG VERSION 5.1, Round 11 (2006-07)
NHCDC Reporting Standards http://www.ihpa.gov.au/internet/ihpa/publishing.nsf/Content/EC0666091A19EBB1CA257B9B0083827A/$File/HospitalPatientCostingStandards_v2_Final_June%202011.pdf
In summary - Why do we need clinical costing? • Accurately value products – eg DRG’s for funding • Costweights for funding and payment • Activity analysis in weighted activity terms • Benchmark our hospital against others and over time • Properly manage performance – care profiles • Set achievement targets – ‘match the above average performers over the next two years’