Download
1 / 1
10 likes | 134 Views
“ CONCURRENT CHEMORADIATION ( CChRT ) FOR STAGE III NON-SMALL CELL LUNG CANCER ( NSCLC ): A PHASE II STUDY FROM GALICIAN LUNG CANCER GROUP ”

E N D
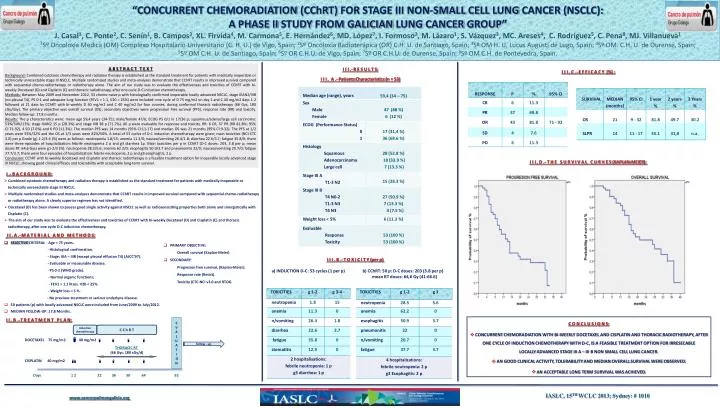
“CONCURRENTCHEMORADIATION (CChRT) FOR STAGE III NON-SMALL CELLLUNG CANCER (NSCLC):A PHASE II STUDYFROMGALICIAN LUNG CANCERGROUP” J. Casal1, C. Ponte2, C. Senín1, B. Campos3, XL. Firvida4, M. Carmona5, E. Hernández6, MD. López7, I. Formoso2, M. Lázaro1, S. Vázquez3, MC. Areses4, C. Rodríguez5, C. Pena8, MJ. Villanueva11Sº Oncoloxía Medica (OM) Complexo Hospitalario Universitario (C. H. U.) de Vigo, Spain; 2Sº Oncoloxia Radioterápica (OR) C.H. U. de Santiago, Spain; 3Sº OM H. U. LucusAugusti de Lugo, Spain; 4Sº OM. C.H. U. de Ourense, Spain;5Sº OMC.H. U. de Santiago, Spain; 6Sº ORC.H.U. de Vigo, Spain; 7Sº ORC.H.U. de Ourense, Spain; 8Sº OMC.H. de Pontevedra, Spain. A B S T R A C T T E X T Background:Combinedcytotoxicchemotherapy and radiationtherapyisestablished as the standard treatmentforpatientswithmedically inoperable ortechnicallyunresectablestage III NSCLC. Multiplerandomizedstudies and meta-analysesdemonstratethatCChRTresults in improvedsurvivalcomparedwithsequentialchemo-radiotherapyorradiotherapyalone. Theaim of ourstudywastoevaluatetheeffectiveness and toxicities of CChRTwithbi-weeklyDocetaxel (D) and Cisplatin (C) and thoracicradiotherapy, afteronecycle D-C inductionchemotherapy. Methods:BetweenMay 2009 and November 2012, 53 chemo-naive p withhistologicallyconfirmed inoperable locallyadvancedNSCLC, stage IIIAN2/IIIB (no pleural T4), PS 0-1 and adequatelungfunction (FEV1 > 1.1, V20 < 25%) wereincluded: onecycle of D 75 mg/m2 onday 1 and C 40 mg/m2 days 1-2 followed at 21 daysbyCChRTwithbi-weekly D 40 mg/m2 and C 40 mg/m2 forfourcourses, duringconformalthoracicradiotherapy (66 Gys, 180 cGy/day). Theprimaryobjectivewasoverallsurvival (OS); secondaryobjectiveswereprogression free survival (PFS), response rate (RR) and toxicity. Median follow-up: 17,8 months. Results:The p characteristicswere: mean age 59,4 years (34-75); male/female 47/6; ECOG PS 0/1 in 17/36 p; squamous/adeno/largecell carcinoma: 53%/34%/13%; stage IIIAN2 15 p (28.3%) and stageIIIB 38 p (71.7%). All p were evaluable for response and toxicity. RR: 6 CR, 37 PR (RR 81.8%; 95% CI:71-92), 4 SD (7.6%) and 6 PD (11.3%). The median PFSwas 14 months (95% CI:11-17) and median OS was 21 months (95% CI:9-32). ThePFS at 1/2 yearswere 55%/32% and the OS at 1/3 yearswere 82%/50%. A total of 53 cycles of D-C inductionchemotherapyweregiven; maintoxicities (NCI-CTC 3.0) per p Grade (g) 1-2/3-4 (%) were as follows: neutropenia 1.8/15; anemia 11.3/0; nausea/vomiting 26.4/1.8; diarrhea 22.6/3.7; fatigue 35.8/0; therewerethreeepisodes of hospitalization: febrile neutropenia 2 p and g3 diarrhea 1p. Maintoxicities per p in CChRT (D-C doses: 203, 3.8 per p; mean doses RT: 64,6 Gys) were g1-2/3 (%): neutropenia 28.3/5.6; anemia 62.2/0; esophagitis 50.9/3.7 and pneumonitis 32/0; nausea/vomiting 20.7/0; fatigue 37.7/3.7; therewerefourepisodes of hospitalization: febrile neutropenia, 2 p and g3 esophagitis, 2 p. Conclusion:CChRTwithbi-weeklyDocetaxel and Cisplatin and thoracicradiotherapyis a feasibletreatmentoptionfor inoperable locallyadvancedstage III NSCLC, showinggoodclinicalefficacy and tolerabilitywithacceptablelong-termsurvival. I II .- R E S U L T S: I II . A .- PatientsCharacteristics (n = 53) I II . C .- E F F I C A C Y (%) : I II . D .- T h e s u r v i v a l c u r v e s (Kaplan-Meier): • I .- B A C K G R O U N D: • Combinedcytotoxicchemotherapy and radiationtherapyisestablished as the standard treatmentforpatientswithmedically inoperable or • technicallyunresectablestage III NSCLC. • Multiplerandomizedstudies and meta-analysesdemonstratethatCChRTresults in improvedsurvivalcomparedwithsequentialchemo-radiotherapy • orradiotherapyalone. A clearly superior regimen has not identified. • Docetaxel(D) has beenshowntoposessgood single activityagainstNSCLC as well as radiosensizitingpropertiesbothalone and sinergisticallywith • Cisplatin (C). • Theaim of ourstudywastoevaluatetheeffectiveness and toxicities of CChRTwithbi-weeklyDocetaxel (D) and Cisplatin (C) and thoracic • radiotherapy, afteronecycle D-C inductionchemotherapy. • I I . A .- M a t e r i a l a n d M e t h o d s: • SELECTIVECRITERIA: - Age < 75 years. • - Histologicalconfirmation. • - Stage: IIIA – IIIB (except pleural effusion T4) (AJCC’97). • - Evaluable ormeasurabledisease. • - PS 0-1 (WHO grade). • - Normal organicfunctions; • - FEV1 > 1.1 litres. V20 < 25%. • - Weightloss < 5 %. • - No previoustreatmentorseriousunderlynedisease. • 50patients (p) withlocallyadvancedNSCLCwereincludedfrom June/2009 toJuly/2012. • MEDIAN FOLLOW-UP: 17,8 Months. • PRIMARYOBJECTIVE: • Overallsurvival (Kaplan-Meier) • SECONDARY: • Progresion free survival, (Kaplan-Meier). • Response rate (Recist). • Toxicity (CTC-NCI v3.0 and RTOG. I II . B .- T O X I C I T Y (per p) a) INDUCTION D-C:53 cycles(1 per p) b) CChRT: 50 p: D-C doses: 203 (3.8 per p) mean RT doses: 64,6 Gy (41-66.6) I I . B .- T R E A T M E N T P L A N: DOCETAXEL75 mg/m2 40 mg/m2 THORACICRT(66 Gys: 180 cGy/d) CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 • C O N C L U S I O N S: • CONCURRENTCHEMORADIATIONWITH BI-WEEKLYDOCETAXEL AND CISPLATIN AND THORACICRADIOTHERAPY, AFTERONECYCLE OF INDUCTIONCHEMOTHERAPYWITH D-C, IS A FEASIBLE TREATMENT OPTION FORIRRESECABLE • LOCALLY ADVANCED STAGE III A – III B NON SMALL CELL LUNGCANCER. • AN GOOD CLINICALACTIVITY, TOLERABILITY AND MEDIAN OVERALLSURVIVALWEREOBSERVED. • An acceptable long term survival was ACHIEVED. E V A L U A T I O N Induction chemotherapy C C h R T follow - up IASLC, 15TH WCLC 2013; Sydney: # 1010 www.cancerpulmongalicia.org