Download
1 / 1
10 likes | 89 Views
Daily Vitamin D Supplementation in the Active Surveillance of Low-Risk Prostate Cancer Medical University of South Carolina, Charleston, SC L. Cannick, MD; D.T. Marshall, MD, MS; S.J. Savage, MD; L.H. Ambrose, RN; Elizabeth Garrett-Mayer, PhD; S. Gattoni-Celli, MD. Abstract :

E N D
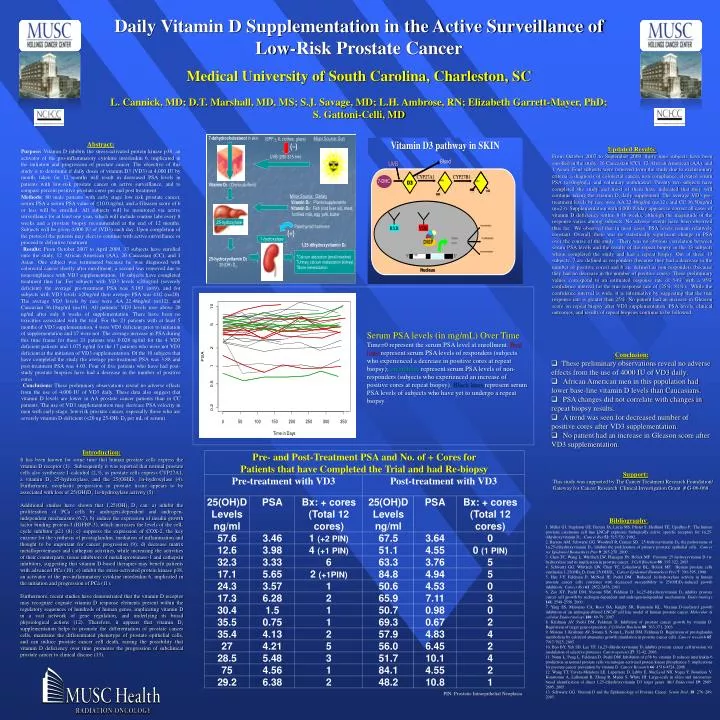
Daily Vitamin D Supplementation in the Active Surveillance of Low-Risk Prostate Cancer Medical University of South Carolina, Charleston, SC L. Cannick, MD; D.T. Marshall, MD, MS; S.J. Savage, MD; L.H. Ambrose, RN; Elizabeth Garrett-Mayer, PhD; S. Gattoni-Celli, MD Abstract: Purpose: Vitamin D inhibits the stress-activated protein kinase p38, an activator of the pro-inflammatory cytokine interleukin 6, implicated in the initiation and progression of prostate cancer.The objective of this study is to determine if daily doses of vitamin D3 (VD3) at 4,000 IU by mouth, taken for 12 months will result in decreased PSA levels in patients with low-risk prostate cancer on active surveillance, and to compare percent positive prostate cores pre and post treatment. Methods: 80 male patients with early stage low risk prostate cancer, serum PSA a serum PSA value of ≤10.0 ng/ml, and a Gleason score of 6 or less will be enrolled. All subjects will be monitored via active surveillance for at least one year, which will include routine labs every 8 weeks and a prostate biopsy recommended at the end of 12 months. Subjects will be given 4,000 IU of (VD3) each day. Upon completion of the protocol the patients may elect to continue with active surveillance or proceed to definitive treatment. Results: From October 2007 to April 2009, 33 subjects have enrolled onto the study, 12 African American (AA), 20 Caucasian (CC), and 1 Asian. One subject was terminated because he was diagnosed with colorectal cancer shortly after enrollment; a second was removed due to noncompliance with VD3 supplementation. 10 subjects have completed treatment thus far. For subjects with VD3 levels <20ng/ml (severely deficient) the average pre-treatment PSA was 5.183 (n=9), and for subjects with VD3 levels >20ng/ml their average PSA was 4.02 (n=20). The average VD3 levels by race were AA 22.48ng/ml (n=12), and Caucasian 36.18ng/ml (n=19). All patients’ VD3 levels rose above 20 ng/ml after only 8 weeks of supplementation. There have been no toxicities associated with the trial. For the 21 patients with at least 5 months of VD3 supplementation, 4 were VD3 deficient prior to initiation of supplementation and 17 were not. The average increase in PSA during this time frame for these 21 patients was 0.028 ng/ml for the 4 VD3 deficient patients and 1.075 ng/ml for the 17 patients who were not VD3 deficient at the initiation of VD3 supplementation. Of the 10 subjects that have completed the study the average pre-treatment PSA was 3.88 and post-treatment PSA was 4.03. Four of five patients who have had post-study prostate biopsies have had a decrease in the number of positive cores. Conclusions: These preliminary observations reveal no adverse effects from the use of 4,000 IU of VD3 daily. These data also suggest that vitamin D levels are lower in AA prostate cancer patients than in CC patients. The use of VD3 supplementation may decrease PSA velocity in men with early-stage, low-risk prostate cancer, especially those who are severely vitamin D-deficient (<20 ng 25-OH- D3 per mL of serum). Updated Results: From October 2007 to September 2009, thirty nine subjects have been enrolled in the study: 26 Caucasian (CC), 12 African American (AA), and 1 Asian. Four subjects were removed from the study due to exclusionary criteria: a diagnosis of colorectal cancer, non-compliance, elevated serum PSA (>10ng/mL), and voluntary withdrawal. Twenty two subjects have completed the study and most of them have indicated that they will continue taking the vitamin D3 daily supplement. The average VD3 pre-treatment levels by race were AA 22.48ng/ml (n=12), and CC 36.50ng/ml (n=23). Supplementation with 4,000 IU/day appears to correct all cases of vitamin D deficiency within 8-16 weeks, although the magnitude of the response varies among subjects. No adverse events have been observed thus far. We observed that in most cases, PSA levels remain relatively constant. Overall, there was no statistically significant change in PSA over the course of the study. There was no obvious correlation between serum PSA levels and the results of the repeat biopsy in the 13 subjects whom completed the study and had a repeat biopsy. Out of these 13 subjects, 7 are defined as responders (because they had a decrease in the number of positive cores) and 6 are defined as non-responders (because they had no decrease in the number of positive cores). These preliminary values correspond to an estimated response rate of 54% with a 95% confidence interval for the true response rate of (25%, 81%). While the confidence interval is wide, it is informative by suggesting that the true response rate is greater than 25%. No patient had an increase in Gleason score on repeat biopsy after VD3 supplementation. PSA levels, clinical outcomes, and results of repeat biopsies continue to be followed. Serum PSA levels (in mg/mL) Over Time Time=0 represent the serum PSA level at enrollment. Red lines represent serum PSA levels of responders (subjects who experienced a decrease in positive cores at repeat biopsy); green lines represent serum PSA levels of non-responders (subjects who experienced an increase of positive cores at repeat biopsy). Black lines represent serum PSA levels of subjects who have yet to undergo a repeat biopsy. • Conclusion: • These preliminary observations reveal no adverse effects from the use of 4000 IU of VD3 daily. • African American men in this population had lower base-line vitamin D levels than Caucasians. • PSA changes did not correlate with changes in repeat biopsy results. • A trend was seen for decreased number of positive cores after VD3 supplementation. • No patient had an increase in Gleason score after VD3 supplementation. Introduction: It has been known for some time that human prostate cells express the vitamin D receptor (1). Subsequently it was reported that normal prostate cells also synthesize 1-calcidiol (2,3), as prostate cells express CYP27A1, a vitamin D3 25-hydroxylase, and the 25(OH)D3 1α-hydroxylase (4). Furthermore, neoplastic progression in prostate tissue appears to be associated with loss of 25(OH)D3 1α-hydroxylase activity (5). Additional studies have shown that 1,25(OH)2 D3 can: a) inhibit the proliferation of PCa cells by androgen-dependent and androgen-independent mechanisms (6,7); b) induce the expression of insulin growth factor binding protein-3 (IGFBP-3), which increases the levels of the cell-cycle inhibitor p21 (8); c) suppress the expression of COX-2, the key enzyme for the synthesis of prostaglandins, mediators of inflammation and thought to be important for cancer progression (9); d) decrease matrix metalloproteinases and cathepsin activities, while increasing the activities of their counterparts, tissue inhibitors of metalloproteinase-1 and cathepsin inhibitors, suggesting that vitamin D-based therapies may benefit patients with advanced PCa (10); e) inhibit the stress-activated protein kinase p38, an activator of the pro-inflammatory cytokine interleukin 6, implicated in the initiation and progression of PCa (11). Furthermore, recent studies have demonstrated that the vitamin D receptor may recognize cognate vitamin D response elements present within the regulatory sequences of hundreds of human genes, implicating vitamin D in a vast network of gene regulation, and underlying its broad physiological actions (12). Therefore, it appears that vitamin D3 supplementation helps to promote the differentiation of prostate cancer cells, maintains the differentiated phenotype of prostate epithelial cells, and can induce prostate cancer cell death, raising the possibility that vitamin D deficiency over time promotes the progression of subclinical prostate cancer to clinical disease (13). Support: This study was supported by The Cancer Treatment Research Foundation/ Gateway for Cancer Research Clinical Investigation Grant # G-06-068 Bibliography: 1. Miller GJ, Stapleton GE, Ferrara JA, Lucia MS, Pfister S, Hedlund TE, Upadhya P. The human prostatic carcinoma cell line LNCaP expresses biologically active, specific receptors for 1α,25-dihydroxyvitamin D3. Cancer Res 52: 515-520, 1992. 2. Barreto AM, Schwartz GG, Woodruff R, Cramer SD. 25-hydroxyvitamin D3, the prohormone of 1α,25-dihydroxyvitamin D3, inhibits the proliferation of primary prostatic epithelial cells. Cancer res Epidemiol Biomarkers Prev9: 265-270, 2000. 3. Chen TC, Wang L, Whitlach LW, Flanagan JN, Holick MF. Prostatic 25-hydroxyvitamin D-1α-hydroxylase and its implication in prostate cancer. J Cell Biochem88: 315-322, 2003. 4. Schwartz GG, Whitlach LW, Chen TC, Lokeshwar BL, Holick MF. Human prostate cells synthesize 1,25(OH)2 D3 from 25(OH)D3. Cancer Epidemiol Biomarkers Prev7: 391-395, 1998. 5. Hsu J-Y, Feldman D, McNeal JE, Peehl DM. Reduced 1α-hydroxylase activity in human prostate cancer cells correlates with decreased susceptibility to 25(OH)D3-induced growth inhibition. Cancer Res 61: 2852-2856, 2001. 6. Zao XY, Peehl DM, Navone NM, Feldman D. 1α,25-dihydroxyvitamin D3 inhibits prostate cancer cell growthby androgen-dependent and androgen-independent mechanisms. Endocrinology 141: 2548-2556, 2000. 7. Yang ES, Maiorino CA, Roos BA, Knight SR, Burnstein KL. Vitamin D-mediated growth inhibition of an androgen-ablated LNCaP cell line model of human prostate cancer. Molecular & cellular Endocrinology 186: 69-79, 2007. 8. Krishnan AV, Peehl DM, Feldman D. Inhibition of prostate cancer growth by vitamin D: Regulation of target gene expression. J Cellular Biochem88: 363-371, 2003. 9. Moreno J, Krishnan AV, Swami S, Nonn L, Peehl DM, Feldman D. Regulation of prostaglandin metabolism by calcitriol attenuates growth stimulation in prostate cancer cells. Cancer research 65: 7917-7925, 2005. 10. Bao BY, Yeh SD, Lee YF. 1α,25-dihydroxyvitamin D3 inhibits prostate cancer cell invasion via modulation of selective proteases. Carcinogenesis 27: 32-42, 2006. 11. Nonn L, Peng L, Feldman D, Peehl DM. Inhibition of p38 by vitamin D reduces interleukin-6 production in normal prostate cells via mitogen-activated protein kinasephosphatase 5: implications for prostate cancer prevention by vitamin D. Cancer Research 66: 4516-4524, 2006. 12. Wang TT, Tavera-Mendoza LE, Laperriere D, Libby E, MacLeod NB, Nagai Y, Bourdeau V, Konstorum A, Lallemant B, Zhang R, Mader S, White JH. Large-scale in silico and microarray-based identification of direct 1,25-dihydroxyvitamin D3 target genes. Mol Endocrinol19: 2685-2695, 2005. 13. Schwartz GG. Vitamin D and the Epidemiology of Prostate Cancer. Semin Dial, 18: 276–289, 2005. PIN: Prostatic Intraepithelial Neoplasia