Download
1 / 3
30 likes | 92 Views
Motivation. We wish to study the effect of genotype, measured at cohort baseline on incident disease during follow-up. Question: should we exclude cohort members with prevalent disease at baseline?

E N D
Motivation • We wish to study the effect of genotype, measured at cohort baseline on incident disease during follow-up. Question: should we exclude cohort members with prevalent disease at baseline? • We usually say that we should: “cohort members with prevalent disease at baseline are not at risk for incident disease during follow-up—by definition”. Therefore: exclude them. • Here, I try to examine the wisdom of that exclusion from the DAG perspective. Notice that restriction to disease-free at baseline is essentially conditioning on a variable called “prevalent disease status”.
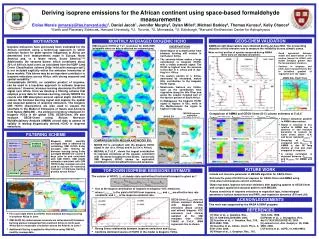
Imagine our cohort as identified at birth Unknown causes of the disease Survival Recovery Duration Inc. disease (by time 1) Prev. disease (baseline disease status) Inc. disease (since baseline) Genotype (true) ? Genotype (measured) Cohort birth Cohort baseline Assumptions: 1) The gene is a cause of the disease; 2) The gene affects survival/recovery/disease duration only through its effect on incident disease; 3) We don’t know all causes of the disease We try to estimate the magnitude of the blue arrow (the genotype’s effect during cohort follow-up) See analysis on the next slide.
Analysis of the DAG • The marginal association of genotype and incident disease during cohort follow up reflects three cause-and-effect pathways: The blue arrow pathway and two green arrow pathways. • The segment “prevalent disease incident disease (since baseline)” is, in part, human-made causation. A person with prevalent disease must take the value “no incident disease since baseline”. And a person without prevalent disease may or may not become incident disease. There is an inverse association between the two variables. • I think people condition on prevalent disease (denoted by a box) in order to block the green arrow pathways, and estimate the “direct” effect alone (blue arrow). The green-arrow pathways may create bias because the genotype could increase incident disease by time 1, increase prevalent disease at cohort baseline, and thereby decrease incident disease since baseline. • BUT: notice that prevalent disease is a collider on paths from genotype to incident disease since baseline. Genotype and unknown causes of the disease collide at prevalent disease. We open these paths by conditioning (by restriction to disease-free at baseline), and thereby add a component of a spurious association between genotype and incident disease since baseline. (Genotype and those unknown causes may become associated within the stratum called “disease-free at baseline”). By the way, this may be another example of the pitfalls of conditioning on an effect of the exposure. • Notice that these “unknown causes” are not “unknown confounders”. They are simply “unknown causes”, which always exist unless we are willing to assume that all causes were known and measured… • So, maybe it is better to include prevalent disease in some cohort studies??? Maybe it’s better to recruit them and include them in cohort analysis of incident disease? • My questions: Is the DAG correct? Have I drawn the arrows correctly? If so, is my analysis correct? Has this problem been described before in the genetic epi literature or elsewhere?