Download
1 / 9
100 likes | 124 Views
NOROVIRUS AT ARROWE PARK HOSPITAL WINTER 2009-2010. 850 BED DGH WITH RANGE OF SUBSPECIALITIES LAST MAJOR NORO PROBLEM 2001/02 OVERALL WELL FUNTIONING HOTEL SERVICES AND ESTATES, AND GOOD COOPERATION WITH ICPT 6 WARDS DIRECTORATE OF MEDICINE FOR THE ELDERLY. THE OUTBREAK.

E N D
NOROVIRUS AT ARROWE PARK HOSPITAL WINTER 2009-2010 • 850 BED DGH WITH RANGE OF SUBSPECIALITIES • LAST MAJOR NORO PROBLEM 2001/02 • OVERALL WELL FUNTIONING HOTEL SERVICES AND ESTATES, AND GOOD COOPERATION WITH ICPT • 6 WARDS DIRECTORATE OF MEDICINE FOR THE ELDERLY Dr Paul Shears DIPC Wirral University Teaching Hospital
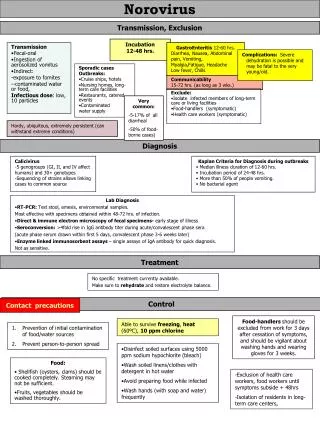
THE OUTBREAK • First cluster of cases of acute diarrhoea/vomiting last week in December on a DME ward: norovirus confirmed using loop-amp pcr kit • Cases continued to increase for next three weeks • Then, mid December, number of case fell, reilef • Few days before Christmas cases increased, leading to crisis bed meetings on Christmas Eve • Outbreak then continued through January, February, March, finally ending early April Dr Paul Shears DIPC Wirral University Teaching Hospital
THE “OUTBREAK” Dr Paul Shears DIPC Wirral University Teaching Hospital
BED DAYS LOST Total bed days lost 1689 Dr Paul Shears DIPC Wirral University Teaching Hospital
Estimated additional financial costs to the Trust: • Bed days: 1689 X £381/day = £645,000 • Staff sickness: 327 staff days = £30, 000 • Hotel Services: (Mostly additional staff hours): = £40,000 • Linen/laundering: = £9,000 • Bottled water = £5000 • Laboratory: Loopamp = £9500, Ridaquick= £500 • BMS/ICN/DIPC time not costed (but should be) • Total cost: £739,000 Dr Paul Shears DIPC Wirral University Teaching Hospital
“Non-financial” costs to the Trust • Public and media concerns • Extreme pressures on bed bureau and nurse managers • Consultant hassles • Extra apparent cases of C.difficile • Time displaced from other urgent infection control activities, particularly MRSA and C.difficile action Dr Paul Shears DIPC Wirral University Teaching Hospital
The Infection Control strategies implemented • Attempted to keep beds open by not closing whole ward when first cases occurred if they were in same area, but required strict ward hygiene • Enhanced hygiene, hand washing etc by all staff………… • Testing new cases of diarrhoea on same ward, and if noro –ve, keeping that area open • Ward closed to new admissions • Restricted visiting • Bottled water (? Evidence) • No transfers from ward • If ward closed, closed till 48hr after last symptomatic case, but sometimes diffcult with bed pressures • Ward “infection control clean” before re-opening Dr Paul Shears DIPC Wirral University Teaching Hospital
Infection control issues to be addressed • Should we have closed complete ward once first cases occurred, would have blocked more beds in short term, but may have shortened outbreak • Why was it continuing: • ? Visitors bringing it in, ? Asymptomatic patients admitted, ? Asymptomatic staff, ? Environment • Why repeated clusters after cleaning, cleaning assumes noro in environment, is it?, if so, was cleaning not effective • Communication with medical staff Dr Paul Shears DIPC Wirral University Teaching Hospital
Do we understand the epidemiology of norovirus • Duration of infectivity • Routes of transmission • Environmental reservoir • Different genotypes • How actually transmitted from patient to patient • Bottled water, false security? • Can patients get repeat infections • Etc Dr Paul Shears DIPC Wirral University Teaching Hospital