Download
1 / 28
290 likes | 304 Views
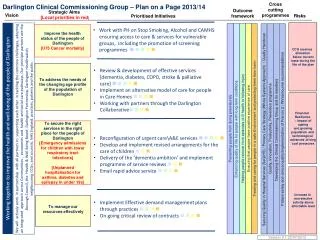
The Integrated County Durham & Darlington NHS Foundation Trust: Developing a Clinical Strategy. Second Stakeholder Event 31 March 2011. Welcome. Stephen Eames. Agenda. Introduction: What we have done since the event on 27 January Purpose of the day Workshops

E N D
The Integrated County Durham & Darlington NHS Foundation Trust:Developing a Clinical Strategy Second Stakeholder Event 31 March 2011
Welcome Stephen Eames
Agenda • Introduction: • What we have done since the event on 27 January • Purpose of the day • Workshops • Part one: outlining and testing proposals • Part two: high priorities and quick wins • Feedback • Next steps
From tomorrow… • …an acute and community Foundation Trust for County Durham and Darlington • …more integrated, better co-ordinated care for patients • …helping the health and social care system work together more effectively
Key messages • There is only one process – and you are part of it! • This is about hospital and community services, not just hospital services! • No decisions have been made! • PCT proposal for hyper-acute stroke must be subject to consultation • However – there are pressures which need to be addressed
Introduction Dr Robin Mitchell
27 January – a reminder Developing vision – an opportunity “to shift the centre of gravity from hospital to community and develop fully integrated care pathways”.
What we have done since 27 January • Summarised stakeholder feedback • Staff feedback at roadshows • Internet survey • Established small workstream teams • Reviewed design principles based on discussion on 27 January • Developed proposals for consideration today
You said: 27 January – summary feedback Safe and high quality care Care delivered closer to home Do more to meet needs of the elderly Improved influence & Engagement What we need to do Accessible, efficient and high quality emergency care More care delivered closer to home / in community Demonstrable excellence of care for LTC/older people/stroke /EOL Integrated sustainable womens & childrens services Improved prevention Leading edge planned care for CD&D Clinical services which are fully integrated with local health and social care networks Joint working to reduce stays / and readmissions Invest in the infrastructure to make it happen Needs of our population Focus on Quality, outcomes, safety Deliver financial sustainability & Commissioning intentions Development of new consortia Emerging policy and guidance Large flexible workforce Alliances with partners & pathfinders Innovation and Improvement Tcs integration - major pathways in one organisation Local opportunities Distance between in-patient sites Decreasing number of medics Increasing demographic pressure Reduction in number of hospital beds lo Local constraints
You said: revised design principles • Right person, right place, right time • senior clinician review as early in the pathway as possible where required • Emphasis on prevention first • Support the reduction of health inequalities • Care closer to home • Integrated pathways designed to deliver flexible, co-ordinated services’ • Making the best use of existing facilities • Services supported by high quality information for patients and staff • Effective working with care partners • Invest to save
Purpose of today • Outlining and testing emerging proposals • Agreeing high priorities and quick wins • Agreeing next steps
Workshops – part one • Update workshops on work to date • Describe the emerging proposals • Use patient scenarios to test proposals against: • Target outcomes • Design principles
Workshops – part two • High priorities - strategic issues that we need to progress urgently • Quick wins: issues which we can progress now to improve services
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Facilitated discharge – identifying people while in nhosp Who will do that role? How will info get out to the community team> Fully Suppported by the table and the room Long term conditions - heart
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Urgent pathway to prevent admission rollout to south Durham Uniform resp pathway for county and published on map of medicine – led by Alwyn Foden Concerns – staff : training existing staff at all levels – IT! Onwards and upwards! Positive impact on A&E Long term conditions - resp
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Good referral guidelines for disease progression, pathway for minor acute events Patient education – continue with DAFNE Numbers of people with diabetes – IT systems for timely info exchange All in agreement – need true integration Long term conditions - diab
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Dementia – training of all staff who are in contact with older people through elearning etc; information to signpost patients to services, linked to map of medicine; NED champion Priority – single point of access to range of services IT – funding boundaries between organisations – electronic info will reduce boundaries Concerns – funding; need one pot of money across health and social care NB elective work has been drawn into this and will be an enabler Specialty based helplines in the community, to direct patients to right services Older people (inc. elective medical)
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Use of surprise question – 2 way - feeding into GP registers for palliative care Engage in advance care planning with these patients IT – we need timely info, systems which talk to each other; investment in eg 24/7 palliative care in all localities as “invest to save”; capacity and demand for GP registers, esp non malignant; some need for workforce development Stephen Cronin – similar approach required for children Joan Clancy – 24/7 palliative care would reduce panic which leads to A&E and admission Alwyn Foden – map of medicine to support electronic system re single point of contact Lot of expertise already exists in primary care – build on GP and out of hours service. End of life
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Antenatal assessment for vulnerable families Use of existing facilities – identifying the hubs and spokes to facilitate integration Concerns - Skills and training around paed front of house model; nurse led solutions to doctor shortages; every contact a health imp contact; paed support for maternity; IT systems; need to share family issues and make it 24/7 available across agencies Buy in to integ pathway – intrapartum care needs better description Joan Clancy: build on existing teams skills Women’s and children’s
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Implement common assessment proces in UCC and A&E; colocation esp at UHND; integrate therapy teams; signage in A&E; implement see and treat; single mgt structure for clinical teams Priorities: engage NEAS, esp re 111; engage social care and chs – re LTC, older people to avoid admission; 24/7 services in community and social care to avoid admission OOH; workforce plan; understanding why patients come to A&E; pooling UCC and A&E funding would create flexibility Concerns: car parking, lack of 24/7 support; lack of 24/7 UCC in Durham; big public messages; IT, access to systmone; Acute medicine emergency care
Quick win: Any priority issues: Any concerns: Level of support for direction of travel? Pre-opp pathway, universal sign up, feed info to GPs, patient questionnaire – use of telehealth or choose and book? Emergency pathway – consultant advice and guidance for GPs; reduce LOS; more bespoke service; use of diagnostics available to GPs; urology – hosp admission unnecessary – quick win re catheter removal Concern – impact on district nurses: more capacity to avoid putting service at risk; referral from GPs – to avoid referrals which won’t convert surgery Urology pathway quick to implement Concern – care closer to home will use up existing community resources which is available to GPs – avoid unintended consequences, eg admission to hospital Surgery rs
General feedback • Complex picture of needs out of hours and support patients needs
Next steps • Develop a clinical strategy which looks at how we integrate services into a coherent set of proposals • Consider enablers – IM&T, finance, estates, workforce • Consider how we take this forward • Come together again to consider proposals and options – end of May
Thank you! Clinical.strategy@cddft.nhs.uk