Download
1 / 23
240 likes | 305 Views
Intestinal nematodes. [6]- Strongyloides stercoralis. Dwarf-thread Worm. [6]- Strongyloides stercoralis. Morphology. 1- Parasitic Female:. 2.2 mm Long filariform oesophagus1/3 2 uteri with transparent eggs. 2- Free-Living Female:. 1.1mm Rhabditiform oesophagus

E N D
Intestinal nematodes [6]- Strongyloides stercoralis Dwarf-thread Worm
[6]- Strongyloides stercoralis Morphology 1- Parasitic Female: 2.2 mm Long filariform oesophagus1/3 2 uteri with transparent eggs 2- Free-Living Female: 1.1mm Rhabditiform oesophagus 2uteri with single column of eggs 3-Male ( Parasitic or Free-Living) : Many scientists believe that male is only free living and parasitic female reproduce by parthogenesis توالد بكرى 0.7mm Rhab oesophagus Post end curved with2 spicules
Strongyloides stercoralis Cylinder like faecal Facultative parasite In the soil Free-living cycle Indirect cycle ♂ ♀ (free-living) (free-living) In the soil Mature egg In man Parasitic cycle Direct cycle Contains rhabditiform larva 4 moults Optimum environmental conditions Hatching rhabditiform larva 2 moults Unfavorable environmental conditions Infective filariform larva
Larva is swallowed Parasitic Cycle in Man Pulmonary lesion 3rd moult Intestinal lesion Duodenum & upper jejunum Venous blood ♀ ♂ 4th moult Skin lesion parasitic ♀ ♂ Free-livingadult On the ground Rhabditiform larvae in stool Infective filariform larva
Diagnostic Stage Infective Stage Filariform larva Rhabditiform larva In stool of infected man In contaminated soil 250µ long 500-600µ long Rhabditiform oesophagus Filariform oesophagus fills anterior ½ of larva Notched tail end
Pathogenesis and Clinical Picture Skin lesion due to penetration of larvae into the skin. Itching and dermatitis. Lung lesion due to migration of larvae. Verminous pneumonitis minute hemorrhages. (Loeffler’s syndrome) RBCs Inflammatory cells Fever, cough, haemoptysis, dyspnea
Intestinal lesion Duodenitis causing burning epigastric pain with tenderness. Rhabditiform larvae Diarrhoea alternates with constipation Constipation gives enough time for rhabditiform larvae to develop into infective filariform larvae
Adults Strongyloides in small intestine Filariform Larvae Rhabditiform larva penetrate mucosa of large intestine Filariform Larvae penetrate perianal skin after coming out of the anus internal autoinfection external autoinfection
Autoinfection increases worm burden (( كثرة عدد الديدان and leads to persistent infection. Long standing heavy infection causes: Dysentery, malabsorption عدم امتصاص الغذاء, steatorrhoea عدم هضم الدهونand weight loss Larva of S.stercoralis left on skin of buttock or thigh move in the skin at a rate of 5-10 cm / hour causing linear eruption Larva currens Currens: fast running
Disseminated Strongyloidiasis منتشرة Occurs more in patients with impaired immunity Aorta Strongyloides:Opportunistic parasite Venous blood Systemic circulation Larvae penetrate extra intestinal organs Visceral larva migrans
Diagnosis 1- Examination of faeces or duodenal contents for larvae. 2- Examination of sputum for larvae. 3- Eosinophilia. 4- Serological tests. 250µ Treatment Thiabendazole OR Ivermectin Prevention and Control As in Ancylostoma
Verminous Pneumonitis Inflammation of lung tissue due to migration of helmintheslarvae in pulmonary capillaries Occurs in: Migrating schistosomula DO NOT break into alveoli Schistosomiasis: migratingschistosomula Ascariasis: migrating larvae Ancylostomiasis: migrating larvae Strongyloidiasis: migrating larvae Loeffler’s Syndrome X-ray Occurs in: Migrating larvae BREAK OUT from pulmonary capillaries into alveoli Ascariasis Ancylostomiasis Lung shows scattered mottling بقع مبعثرة Strongyloidiasis
Intestinal nematodes [7]- Trichinella spiralis
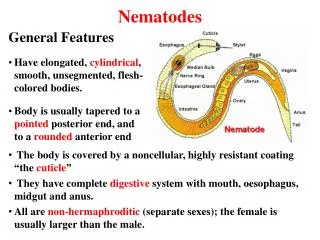
[7]- Trichinella spiralis Trichinosis Trichinella: little hair spiralis: like the spiralمثل الحلزون Geographical distribution: cosmopolitan, especially in pork-eating countries. 2 conical processes ♀ 3 mm long ♂ 1.5 mm long Final host: Man, pigs, rodents. Carnivorus mammals Habitat: Small intestine Intermediate host: Man, pigs, rodents. Young stage (larva) is encysted in muscles of infected man, pig or rodent
Development of Trichinella spiralis in infected Adult worms in intestine die after a short time Man Pig Rodent Larvae in muscles remain for ever Infected muscle contains encysted larva Mucosa of small intestine Each ♀ lays 1500 larvae per day Femaleis larviparous ♂ ♀ ♂ ♀ Muscles are digested in stomach 100µ Blood vessel Larvae penetrate intestinal wall to be carried by blood Active striated muscles Encysted larvae (1000µ)
Infected Pig Infected Rodent Infected Man Diseased rats are eaten by healthy rats Diseased pigs are eaten by healthy pigs Cannibalism الحيوان يأكل لحم جنسه Blind host
Pathogenesis and Clinical Picture Intestinal stage: on the 1st week Patient gives the picture of gastroenteritis. Nausea, vomiting, abdominal cramps and diarrhea ( simulating food poisoning تسمم غذائى ) Larval migration stage: on the 2nd week Fever, oedema of eye lids, myositis and weakness of affected muscles, eosinophilia. Encapsulation stage: on the 3rd week Fever subsides, muscle pain persists Death may occur from myocarditis, pneumonia, encephalitis
Diagnosis Clinically:a history of eating pork with fever, facial oedema and myositis. Laboratory: 1- Muscle biopsy:from deltoid or gastrocnemius to detect the larvae. 2- Eosinophilia:in 3rd to 4th week. 3- Bachman test: (intradermal test) 0.1 cc of 1:10,000 dilution of larva antigen is injected I.D. gives a wheal in 20 minutes in positive cases.
4- Serological tests: by IFAT or ELISA IFAT Ab linked to fluorescent dye Patient’s serum wash wash wash Microscopic examination ELISA Coating with Ag Patient’s serum Ab linked to enzyme substrate Ab detected wash wash wash X ray: shows calcified cysts
Treatment • Mebendazole. Kills the worms releasing a large amount of parasite antigens • Corticosteroids. • Symptomatic treatment: for fever, headache and muscle pain. Prevention and Control • Destruction of rats and proper breeding of pigs. • Heat treatment of garbage fed to swine (pigs). • Meat inspection of slaughter house. • Proper cooking of pork.