Download
1 / 42
2.67k likes | 10.95k Views
COUNTER CURRENT MECHANISM (Concentration Mechanism of Urine). Lecture – 7 Dr. Zahoor . COUNTER CURRENT MECHANISM. Kidney can excrete dilute or concentrated urine depending on body state of hydration Body fluids are isotonic having osmolarity of 300 milliosmoles /liter (mOsm/l)

E N D
COUNTER CURRENT MECHANISM (Concentration Mechanism of Urine) Lecture – 7 Dr. Zahoor
COUNTER CURRENT MECHANISM • Kidney can excrete dilute or concentrated urine depending on body state of hydration • Body fluids are isotonic having osmolarity of 300 milliosmoles/liter (mOsm/l) • Depending on body state of hydration kidney can excrete urine having osmolarity from 100 – 1200 mOsm ( Normal urine Osmolarity is about 500 – 600 mOsm )
COUNTER CURRENT MECHANISM • Concentration of urine is the function of juxta -medullary nephron, which has long loop of Henle which goes down deep in the medulla • Also, the vasarecta (capillaries) of juxta medullary nephron follow the same deep loop of Henle • Flow in the both long LH and vasarecta is considered counter current because flow in two limbs of the loop move in the opposite direction
Juxta medullary and cortical nephron
COUNTER CURRENT MECHANISM • Concentration of urine is due to 1. Juxta medullary nephron – long loop of Henle establish (create) the vertical osmotic gradient 2. Vasarecta help to maintain (preserve) this osmotic gradient 3. Collecting duct of all nephrons use the gradient along with hormone vasopressin (ADH) to produce urine of varying concentration 4. Urea also help in urine concentration mechanism • This entire functional organization is known as medullary counter current system
COUNTER CURRENT MECHANISM • We will discuss in detail each point 1- Medullary vertical osmotic gradient - created by loop of Henle is called Counter current multiplier - Long loop of Henle in juxta medullary nephron establishes the vertical osmotic gradient. How?
COUNTER CURRENT MECHANISM • As filtrate is formed, it is isotonic in the PCT, water is reabsorbed in PCT, secondary to Na+ active reabsorption • When isotonic fluid enters the loop of Henle changes occur in the descending and ascending limbs of long henles loop
PROPERTIES OF DESCENDING AND ASCENDING LIMBS OF LH • Descending limb of long LH is highly permeable to water due to AQP – 1 water channel which are always open • Descending limb is not permeable to Na+, therefore, Na+ remains in the descending limb of LHand its concentration (osmolarity) increases • Maximum osmolarity is at the tip of LH which is 1200 mOsm/l
PROPERTIES OF DESCENDING AND ASCENDING LIMBS OF LH • Ascending limb of LH actively transports NaCl out of tubular lumen into interstial fluid • Ascending limb is impermeable to H2O • As NaCl leaves and H2O remains, osmolarity decreases in the ascending limb of loop of Henle • Fluid entering the DCT has low osmolarity of 100 mOsm/l
PROPERTIES OF DESCENDING AND ASCENDING LIMBS OF LH IMPORTANT • As Na+ is actively transported out of ascending limb of LH, concentration increases in the interstitial fluid surrounding the loop of Henle • This increased concentration in the interstitial fluid achieved by loop of Henle is known as Counter Current Multiplication
Vertical Osmotic Gradient In The Renal Medulla • A large, vertical osmotic gradient is established in the interstitial fluid of the medulla
BENEFITS OF COUNTER CURRENT MULTIPLICATION • What is the benefit of fluid getting concentrated in the descending limb of LH and again diluted in the ascending limb of LH? Benefits are - It establishes a vertical osmotic gradient in the medullary interstial fluid - This gradient is used by collecting ducts to concentrate the tubular fluid (urine)
BENEFITS OF COUNTER CURRENT MULTIPLICATION • As fluid is hypotonic as it enters CT, the kidney can excrete dilute urine or it can be concentrated in the CT. How ? - ADH controls water reabsorption in DCT and CT. About 20% of H2O enters DCT and CT, and it is under control of ADH NOTE - We know that in PCT 65% of water is reabsorbed and in LH 15% of water is reabsorbed
2. ROLE OF VASOPRESSIN (ADH) • As fluid enters the CT, it is hypotonic. • For water reabsorption to occur in CT, Two criteria must be met: 1. Osmotic Gradient across the CT – it is there as interstial fluid is concentrated by LH- counter current multiplication 2. Collecting tubule must be permeable to water, it is there due to presence of ADH (normally DCT and CT are impermeable to H2O)
ROLE OF VASOPRESSIN (ADH) • How ADH increases the permeability of DCT and CT? - ADH binds to V2 receptors, which are G-protein receptors which activate cAMP, second messenger in DCT and CT - It increases the permeability to water by insertion of Aquaporins (AQP-2 water channels in the luminal membrane)
Mechanism of action of ADH
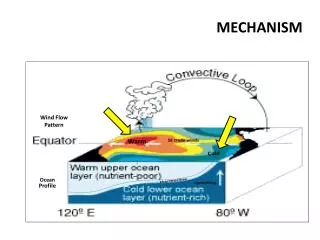
3. VASARECTA – COUNTER CURRENT EXCHANGER • We will study vasarecta, which works as counter current exchanger and preserves the medullary osmotic gradient, created by LH • Vasarecta are freely permeable to NaCl and H2O. As blood passes down the descending limb of vasarecta, it picks up salt and loses H2O, till it is hypertonic at the bottom(1200 mOsm ).
VASARECTA – COUNTER CURRENT EXCHANGER • As blood flows up in the ascending limb of vasarecta, salt moves into the interstium and water enters the vasarecta, therefore, concentration falls in the ascending limb of vasarecta ( 300-350 mOsm ). • This passive exchange of NaCl and H2O in the descending and ascending limbs of vasarecta and interstial fluid is known as counter current exchange
The VasaRectaPreserve Hyperosmolarity of Renal Medulla • The vasa recta • serve as • countercurrent • exchangers • Vasa recta blood • flow is low • (only 1-2 % of • total renal • blood flow)
IMPORTANT • Loop of Henle – counter current multiplier establishes the concentration gradient in the medullary interstitial fluid. • Vasarecta – counter current exchanger maintains the concentration gradient in the medullary interstitial fluid.
4. ROLE OF UREA IN CONCENTRATION OF URINE • Urea contributes to hyper osmotic renal medullary interstial fluid and to concentrated urine. How ? - Urea is absorbed in PCT – 50% - 50% urea comes to DCT and CT, they are not permeable to urea but collecting duct in the inner medulla is permeable
ROLE OF UREA IN CONCENTRATION OF URINE- UREA CYCLE - When water is reabsorbed in DCT and CT under action of ADH, urea is more concentrated - Urea diffuses from CT in the inner medullary region and contributes to the concentration of medullary interstial fluid - Increased urea present in the interstial fluid diffuses into loop of Henle (descending and ascending limbs) and then to DCT and CT, therefore, recirculates many times before it is excreted – called Urea Cycle
Recirculation of Urea Absorbed from Medullary Collecting Duct into Interstitial Fluid Figure 28-5; Guyton and Hall
MICTURITION REFLEX • Micturition or Urination is the process by which bladder is emptied, and is governed by two mechanism: 1. Micturition Reflex 2. Voluntary Control
MICTURITION REFLEX • Micturition Reflex • It is initiated when stretch receptors in the urinary bladder are stimulated • Bladder can accommodate 250 – 400ml of urine • Urine urge is felt when there is 150ml of urine in the bladder
Normal Cystogram There are 3 phases of vesicular pressure changes Initial 10 cm of H2O rise in pressure for 10-50 ml of urine collection Second phase last until the bladder volume is 400ml Third phase shows the sharp rise in the intravesicle pressure Micturition contractions begin to appear at a urine volume about 150 ml. Desire to void urine occurs when the bladder is full.
MICTURITION REFLEX • When amount of urine increases, there is greater distension – afferent impulses from stretch receptors go to spinal cord via pelvic nerves. • Center in the spinal cord is S2,3,4 • Efferent impulses pass via parasympathetic nerves to the bladder • Parasympathetic supply causes bladder smooth muscle to contract and urine is expelled through urethra by force of bladder smooth muscle contraction IMPORTANT – Micturition reflex is spinal reflex
MICTURITION REFLEX • Voluntary Control of Micturition Micturition is spinal reflex , but facilitated and inhibited by higher Brain centers. - Voluntary Control is done by tightening the external uretheral sphincter and pelvic diaphragm , through pudendal nerve by impulses coming from brain, pons and cerebral cortex to the spinal cord
APPLIED Urinary Incontinence • Urinary Incontinence is loss of voluntary control over urination, therefore, inability to prevent discharge of urine • Cause – spinal cord injury to S2,3,4
RENAL FAILURE • Renal Failure causes kidney functions to be affected • Causes of Renal Failure 1. Infections – urinary tract infection 2. Toxic agents e.g. lead, arsenic, pesticides 3. Drugs – aspirin 4. Immune response glomerulonephritis, following post streptococcal throat infection 5. Kidney stone, tumor, enlarged prostate gland
RENAL FAILURE • Renal failure maybe - Acute Renal Failure - Chronic Renal Failure • Acute Renal Failure – sudden with decreased urinary output, less than 500ml per day • Chronic Renal Failure – slow progressive loss of renal function. It is not reversible
IMPORTANT • Only 25% of kidney tissue is needed to adequately maintain all the functions of kidney • When 75% of kidney tissue is destroyed then loss of kidney function is noticeable • End stage renal failure – when 90% of kidney function is lost
CHRONIC RENAL FAILURE (CRF) • Chronic renal failure can cause - Uremia (increased blood urea level) - Metabolic acidosis - Hyperkalemia - Na+ imbalance - Hypertension - Edema (loss of plasma protein) - Anemia (decreased erythropoietin) • Treatment for CRF - Dialysis - Kidney transplantation
What You Should Know About This Lecture • Describe the factors that determine the ability of loop of Henle to create osmotic medullary gradient • Identify countercurrent multiplier and countercurrent exchange systems in concentrating and diluting urine • Explain changes in osmolarity of tubular fluid in the various segments of the loop of Henle when concentrated urine is being produced. • Describe the role of ADH on the ability of the kidney to produce either a dilute or a concentrated urine. • Micturition reflex.