Download
1 / 8
80 likes | 208 Views
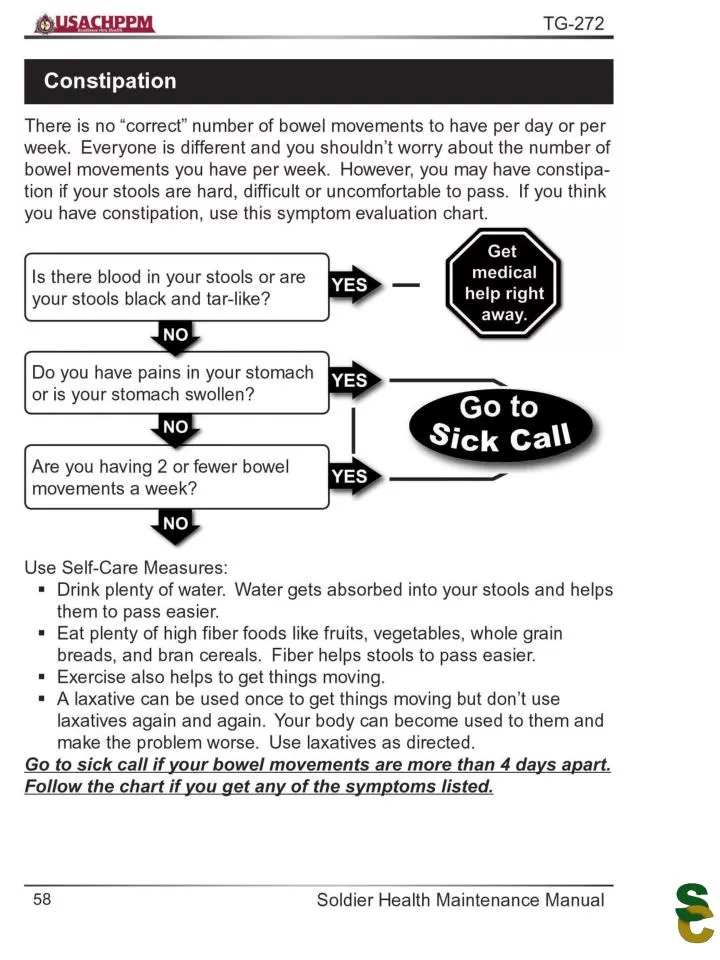
Important Points. Up to five OTC drugs can be issued at one time. All must relate to the chief complaint or identified symptom. Soldiers cannot use the same complaint for two consecutive self-care visits. OTCs cannot be shared with buddies.

E N D
Important Points • Up to five OTC drugs can be issued at one time. All must relate to the chief complaint or identified symptom. • Soldiers cannot use the same complaint for two consecutive self-care visits. • OTCs cannot be shared with buddies. • Soldiers can use the Self-care Program or Sick call at different times and in different situations. • If soldiers are very sick or badly hurt, they must get medical help right away and tell their Drill Sergeant.
Sample Green Sheet TROOP MEDICAL CLINIC (TMC) SELF-CARE PROGRAMTREATMENT OPTIONS FOR SYMPTOMS/CONDITIONS I am aware that I am participating in a self-care program. I understand that to properly perform self-care and safely treat any symptom(s) of conditions(s) that I may have during training I must follow the symptom evaluation charts. I also understand that I am responsible for carefully following the directions for use of any medication received through this program. I verify that I have read the self-care decision guide and the recommendations provided therein. I also verify that I am requesting treatment options(s) voluntarily. I also agree that I will not share medication with anyone and that I will be the sole user. What allergies, to include medications, do you have?_________________________________________ What medicines are you presently taking? ______________________________________________ Print Name Print SSN Date Signature Unit: Sex: M F INSTRUCTIONS: After reading the Soldier Health Maintenance Manual and identifying the proper treatment option(s), find the symptom(s)/condition(s) that you have on the list below. Circle it. Then follow the line across to find the treatment option(s) for your symptom(s)/condition(s). Circle the treatment you would like to receive. Request the identified treatment option(s) from the Consolidated Troop Medical Clinic Pharmacy. Treatment requests will be limited to five items. NOTE: You can select Daytime OR Robo DM liquid but NOT BOTH. You can select Daytime OR SudaGest, but NOT BOTH.
SYMPTOM/CONDITION:TREATMENT OPTION Acne . . . . . . . . . . . . . . . . . . . . . . . . Medication (Benzoyl Peroxide) Allergies & Hay Fever . . . . . . . . . . . . . . . .SudaGest Decongestant (Pseudoephedrine)* Athletes Foot . . . . . . . . . . . . Miconazole Nitrate Antifungal Cream Blisters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Mole Skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Band-Aid . . . . . . . . . . . . . . . . . . . . . . Bacitracin Antibiotic Ointment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Baby Powder (Talc) Constipation . . . . . . . . . . . . . . . . . . . . . . . . . . Genasoft (Ducosate) Cough with congestion . . . . . . . . . . . . . . . . . . . . . . . . . . . Daytime* Cough (dry) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Robo DM liquid* Cut or Scrape . . . . . . . . . . . . . . . . . Bacitracin Antibiotic Ointment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Band-Aid Diarrhea . . . . . . . . . . . . . . . . . . . . . . . . Anti-Diarrheal (Loperamide) Earache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Ibuprofen Tablets Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Ibuprofen Tablets Heat Rash . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Baby Powder (Talc) Insect Bite . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Calamine Lotion . . . . . . . . . . . . . . . . . . Cortaid Cream (Hydrocortisone) Jock Itch . . . . . . . . . . . . . . . Miconazole Nitrate Antifungal Cream . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Baby Powder (Talc) Muscle Pain & Inflammation . . . . . . . . . . . . . . . .Ibuprofen Tablets Nasal or Sinus Congestion (without cough) . . . . . . . . . . SudaGest Decongestant (Pseudoephedrine)* Poison Ivy/Oak/Sumac . . . . . . . . Cortaid Cream (Hydrocortisone) PreMenstrual Syndrome . . . . . . . . . . . . . . . . . . . Ibuprofen Tablets Ringworm . . . . . . . . . . . . . . Miconazole Nitrate Antifungal Cream Runny Nose or sneezing . . . . . . . . . . . . . SudaGest Decongestant (Pseudoephedrine) Sore Throat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Cepacol Upset Stomach . . . . . . . . . . . . . . . . . . . . . . . . Maalox Antacid Plus Vaginitis . . . . . . . . . . . . . . . . . . . . . . Gyne-Lotrimin (vaginal insert) SAMPLE
YELLOW SHEETSelf-care Program Evaluation(Program Participant—Soldier) Instructions Please complete Part 1 and Part 2. Your responses are very important to the Self-care Program. This information is completely confidential and will only be used to improve the program. Please write any additional comments at the bottom of the page. Return the completed form to the proper pick-up location. Thank you. Part 1 Date: ___/___/___ Installation: ______________________ Unit: ______________________________ MOS: ______________ Please circle one response for each of the following: Age: 18 – 19 – 20 – 21 – 22 – 23 – 24 – 25 – Over 25 Sex: M F Highest education level completed: GED – High school – Some college – College graduate
Yellow Sheet: Part 2 Please circle one response for each of the following questions. If not sure, leave that question blank. 1.I used the Self-care manual at least once to take care of myself. Yes No 2.I made at least one clinic visit for Self-care using the Green Sheet. Yes No 3.I made at least one clinic visit for regular Sick call. Yes No 4.The Self-care Program helped me to avoid missing training time at least once. Yes No 5.I would feel comfortable following the Self-care steps in the manual if I needed to. Yes No 6.The Self-care Program is a valuable benefit for my own health. Yes No 7.The Self-care training and manual taught me how to take better care of myself. Yes No 8.When I can, I prefer to use the Self-care Program instead of regular Sick call. Yes No 9.The training and manual helped me decide whether to use Self-care or regular Sick call. Yes No 10.The Self-care Program should be available to all soldiers Yes No
Drill Sergeant’s Role • Ensure soldiers attend the self-care class. • Remind the soldier to follow the Self-care Program procedures. • Distribute the green sheet as requested by soldier. • Green sheets are only to be used by soldiers who have completed the self-care class. • Distribute and collect the yellow sheets at the end of the training cycle for each unit.