Download
1 / 26
270 likes | 411 Views
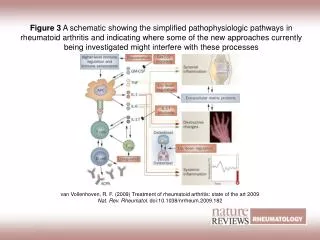
Classical Safety Observations Pooled Safety Data from Tocilizumab Core Studies and Long-term Extension Studies. R van Vollenhoven Karolinska University Hospital, Stockholm, Sweden. Franz Liszt 1811 – 1886. Establishing the long-term safety of TCZ in RA.

E N D
Classical Safety Observations Pooled Safety Data from Tocilizumab Core Studies and Long-term Extension Studies R van VollenhovenKarolinska University Hospital, Stockholm,Sweden
Establishing the long-term safety of TCZ in RA Efficacy and safety of TCZ established in randomised, controlled, Phase III trials1–5 Combination with DMARDs Monotherapy In these 6 to 12-month studies, TCZ was well tolerated Effects of prolonged IL-6R inhibition are unknown 1. Nishimoto N, et al. Ann Rheum Dis 2007; 66:1162–1167. 2. Smolen JS, et al. Lancet 2008; 371:987–997. 3. Genovese MC, et al.Arthritis Rheum 2008; 58:2968–80. 4. Emery P, et al. Ann Rheum Dis 2008; 67:1516–23. 5. Jones G, et al. Ann Rheum Dis 2009 [epub]
Objective To evaluate the long-term safety of TCZ using pooled data from two ongoing, open-label extension studies van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
TCZ Phase III and long-term extension programme 24-week signs and symptoms:AMBITION (N=673)1 MTX-naïve/6 m MTX-free DMARD-IR 24-week signs and symptoms:TOWARD (N=1,220)2 N=2,562 enrolled in long-term extension study as of October 20076 TNF-IR 24-week signs and symptoms:RADIATE (N=499)3 24-week signs and symptoms:OPTION (N=623)4 MTX-IR 2-year progressive joint damage:LITHE (ongoing, N=1,196)5 1. Jones G, et al. Ann Rheum Dis 2009 [epub]. 2. Genovese M, et al. Arthritis Rheum 2008; 58:2968–2980. 3. Emery P, et al. Ann Rheum Dis2008; 67:1516–23. 4. Smolen J, et al.Lancet 2008; 371:987–997. 5. Roche. Data on file. 6. van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670. IR=inadequate responder
More than 90% of patients elected to continue receiving TCZ in extended clinical trials • 2,562 patients enrolled in extension studies (94.3%) • The median TCZ exposure was 1.5 years • Total cumulative TCZ exposure was 3,684.7 patient–years • 360 patients (14.1%) withdrew • 203 (7.9%) due to non-safety reasons • Insufficient therapeutic response (n=75) • Refusal of treatment (n=84) • 157 (6.1%) discontinued treatment due to AEs • Mortality rate: 0.43 per 100 patient–years . van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670. AE=adverse event
More than half of patients received TCZ for at least 1.5 years van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Incidence and type of AEs were comparable to the controlled trials Incidence rate of AEs was 381.6 per 100 patient–years Most common AEs Infections 36% Gastrointestinal (GI) disorders 22% Elevations in lipids and liver enzymes 15% Skin and subcutaneous disorders 14% AEs leading to withdrawal Results of laboratory investigations 1.3% Liver enzyme elevations 1.0% Neoplasms (benign and malignant) 1.1% Infections 0.9% van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
The rate of AEs was highest in the first 6 months and decreased over time 500 400 AEs per100 patient–years (95% CI) 300 200 100 0 Months 0–6 7–12 13–18 19–24 25–30 Patient–years 1,164.7 1,081.9 840.3 456.1 142.9 CI=confidence interval van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
The rate and incidence of SAEs was comparable with the controlled trials • Incidence rate of SAEs was 13.5 per 100 patient–years • SAEs were reported in 393 patients (15.3%) • Most common were infections (5.2%) SAE=serious adverse event van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
The rate of serious adverse events did not increase with prolonged TCZ treatment - - - - 20 15 10 5 0 SAEs per 100 patient–years(95% CI) Months 0–6 7–12 13–18 19–24 25–30 Patient–years 1,081.9 840.3 456.1 142.9 1,164.7 van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
The rate of serious infections was low The rate of serious infections was 3.9 per 100 patient–years Most common infections: Pneumonia 1.2% Cellulitis 0.7% Herpes zoster 0.3% Gastroenteritis 0.2% Diverticulitis 0.2% 4 opportunistic infections* Mycobacterium avium complex infection Pneumocystis jiroveci pneumonia 2 x extrapulmonary mycobacterial infections *2 in controlled studies and 2 in extension studies van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Rate of serious infections with prolonged TCZ treatment 12 10 8 Serious infections per 100 patient–years (95% CI) 6 4 2 0 Months 0–6 7–12 13–18 19–24 25–30 Patient–years 1,081.9 840.3 456.1 142.9 1,164.7 van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Reductions in neutrophil count remain within normal range (6-month safety population) TCZ 8 mg/kg + DMARD (n=1,582) Placebo + DMARD (n=1,170) 12 9 Upper limit of normal Mean neutrophil count (x 109/l) 6 3 Lower limit of normal 0 0 2 4 6 8 10 12 14 16 18 20 22 24 Time (weeks) Roche. Data on file.
Decreased neutrophil counts Transient neutropenia (ANC <1.0 x 109/l) reported in 97 patients (3.8%) 6 patients withdrawn due to ANC <0.5 x 109/l as per protocol No indication that reduced neutrophil counts led to an increased risk of serious infections van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
AST and ALT elevations in patients with normal baseline values ULN=upper limit of normal ALT=alanine transaminase AST=aspartate transaminase van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Shifts in AST and ALT from baseline to highest post-baseline value in TCZ-treated patients AST ALT Normal at baseline (n=2,429) Normal at baseline (n=2,361) 1–3 xULN at baseline (n=131) 1–3 xULN at baseline (n=199) 80 80 60 60 Patients (%) Patients (%) 40 40 20 20 0 0 Normal Normal Normal Normal >3 x ULN >3 x ULN >3 x ULN >3 x ULN 1–3 xULN 1–3 xULN 1–3 xULN 1–3 xULN Highest post-baseline value Highest post-baseline value van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Increases in lipid levels observed with TCZ treatment At the last observation: LDL cholesterol <130 mg/dl at baseline →≥130 mg/dl 37.5% HDL cholesterol <60 mg/dl at baseline → ≥60 mg/dl 21.5% Triglycerides <500 mg/dl at baseline → ≥500 mg/dl 1.3% Elevations in lipid levels were observed with TCZ at the first observation (Week 6) and then stabilised LDL=low density lipoproteinHDL=high density lipoprotein van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Change in LDL cholesterol from baseline to last observation in TCZ-treated patients Baseline LDL cholesterol value (mg/dl): ≥100 – <130 (n=806) <100 (n=820) ≥130 – <160 (n=225) ≥160 (n=248) 100 80 60 Patients (%) 40 20 0 <100 ≥100 – <130 ≥130 – <160 ≥160 LDL cholesterol level at last observation (mg/dl) van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Prolonged TCZ treatment did not increase the risk of cardiovascular events 139 patients (5.4%) reported cardiac disorders, the most frequent being arrhythmias and ischemic events Rate of myocardial infarction was 0.27 per 100 patient–years Rate of stroke was 0.11 per 100 patient–years Both rates were stable over time van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Infusion-related, anaphylactic and hypersensitivity reactions were uncommon in TCZ-treated patients Events that led to withdrawal reported in 13 patients: 6 anaphylactic reactions 3 hypersensitivity reactions 1 report of hypersensitivity to the drug 3 infusion-related reactions All resolved without consequence van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Low immunogenic potential of TCZ • A total of 46 patients (1.6%) treated with TCZ had a positive result in the screening and confirmation assays • Safety-related event-driven testing identified 160 TCZ-treated patients who experienced an infusion-related event • 10 of these patients tested positive for anti-TCZ HAHAs • Hypersensitivity events higher in TCZ 4 mg/kg than 8 mg/kg • 22 TCZ-treated patients were withdrawn from the studies due to insufficient therapeutic response • 14 of these patients tested for the development of anti-TCZ HAHAs • None of these patients tested positive for antibodies with neutralizing activity HAHAs=human anti-human antibodies Ramos-Remus C, et al.ACR 24–29 October 2008; Poster 993.
Gastrointestinal events were uncommon in TCZ-treated patients GI perforations Overall rate of 0.17 per 100 patient–years in Phase III studies (including 6 months of LITHE data) and extension studies Upper GI: 0.02 per 100 patient–years Lower GI: 0.14 per 100 patient–years United Healthcare database: Lower intestinal perforation rate, MTX exposed = 0.11 (0.076–0.152) van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Prolonged TCZ treatment did not increase the rate of malignancies • Malignant neoplasm reported in 53 patients (2.1%) van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.
Pooled Safety Data from Tocilizumab Core Studies and Long-term Extension Studies: Conclusions Incidence and type of AEs were comparable with those in the controlled studies Rates of serious infection and other SAEs did not increase with continued ACTEMRA treatment Rate of serious infections 3.9 per 100 patient–years Low rate of malignancy Long-term safety evaluations ongoing ACTEMRA in combination with DMARDs or as monotherapy was well tolerated over a median treatment duration of 1.5 years van Vollenhoven RF, et al.ACR 24–29 October 2008; Poster 1670.