Download
1 / 21
220 likes | 238 Views
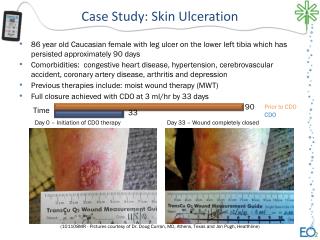
ORAL ULCERATION. Definition – what is an ulcer?. Full thickness breach of the mucosal epithelium Exposes nerve endings underlying the lamina propria Typical symptoms – pain, soreness, discomfort when eating spicy, acidic foods

E N D
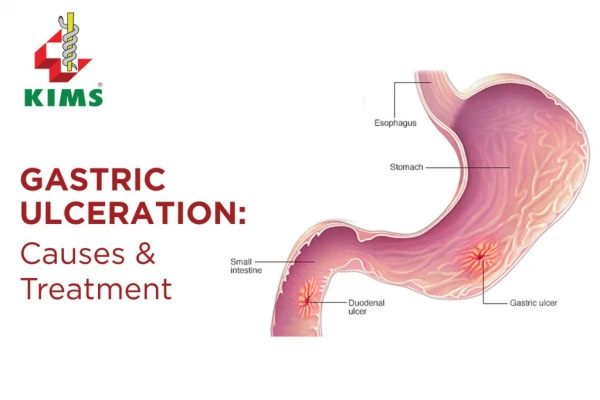
Definition – what is an ulcer? • Full thickness breach of the mucosal epithelium • Exposes nerve endings underlying the lamina propria • Typical symptoms – pain, soreness, discomfort when eating spicy, acidic foods • Can be superficial or extend into tissues underlying the surface epithelium – to submucosa, muscle or periosteum
Classification • Recurrent Apthous Stomatitis (RAS) • Recurrent Oral Ulceration (ROS) – occurring secondary to known or unknown systemic disease/infection • Single episodes of ulceration – trauma, burns, iatrogenic, Squamous Cell Carcinoma • See Table 1 for basic classification overview
Recurrent Apthous Stomatitis (RAS) • Defines recurring episodes of ulceration in healthy individuals • 20% prevalence • Occurring more commonly up to 30yrs but can persist >30yrs • 3 sub-types: Minor, Major or Herpetiform – depending on keratanised/non-keratanised surface and healing characteristics • Features vary with sub-type
Recurrent Oral Ulceration (ROU) • Patients with systemic disease may present with ROU • The aetiology and pathogenesis is directly linked to the underlying disorder • Examples: • Crohn’s Disease • Behcet’s Syndrome • Orofacial Granulomatosis • Leukaemia
Pathogenesis of RAS • Genetic predisposition – positive family history in approx. 1/3 patients • Immunological Factors – T Helper cells & Natural Killer cells predominate in early lesions followed by cytotoxic cells & antibody dependant cellular cytotoxicity
Aetiology - RAS • Genetic predisposition • Immune Deficiency • Hormonal link – fall in progesterone levels during menstrual cycle • Mucosal Integrity • Nutritional/Haematinic Deficiencies – e.g. iron, folate, vitamin B12 • Stress
Features of RAS Minor • Approx 80% of RAS cases • 10-40yrs • Ovoid/round ulcers • <10 mm in diameter • Yellow with red halo • Non-keratinised mucosa e.g. lips, cheek, floor of mouth • Groups of 1-6 ulcers • Heal in <14 days • No scarring
Major • 10% of RAS cases • >10mm • Crops of 2-5 ulcers • Keratinised and non-keratinised mucosa • Heal with scarring • Longer duration – can last several weeks (10-40 days) • More painful than minor • Frequent recurrence
Herpetiform • Common in older groups & females • Recurrent crops of small ulcers – multiple pinhead ulcers (which may look “herpetic”) – 0.5-3mm • Can increase in size to leave large ragged ulcers • Any oral site • Heal without scarring up to 14 days • Extremely painful • Occur continuously
Aetiology - ROU • Pathogenesis directly linked to underlying medical disorder • Secondary to systemic or infectious disease • Haematological – Neutropenia, Leukaemia • Rheumatological – Reactive Arthritis • Gastrointestinal – Chrons disease, ulcerative colitis, OFG • Dermatological – Lichen Planus, Erythema multiforme • Viral – HIV, ANUG, Herpetic gingivostomatitis • Bacterial – Tuberculosis • Behcet’s Syndrome
Behcet’s Syndrome • Auto-inflammatory condition • Apthous like oro-genital ulceration and ocular disease – uveitis • More common in males in 3rd decade • Racial distribution – countries bordering the Mediterranean due to genetic predisposition – HLA tissue types associated HLA-B12, HLA-DR2 and HLA-B51 • Diagnosis based on following criteria – a patient should have one major and two minor of the following: Major Recurrent oral ulceration Recurrent genital ulceration Ocular disease Cutaneous disease Minor Sero-negative arthritis Gastrointestinal disease Vascular Complications Central nervous system involvement
Behcet’s contd… • Oral ulceration similar to RAS • More frequent episodes • More ulcers per crop • Soft palate and oropharynx more commonly involved • More pronounce scarring • Greater resistance to treatment
Reactive Arthritis (Reiter’s Syndrome) • Autoimmine condition • Inflammation of large joints • Inflammation of the eyes – conjunctivitis or uveitis • Urethritis • Mucocutaneous lesions • Patients may present with apthous type ulceration
Single episodes of ulceration • Trauma – burns - chemical, thermal • Iatrogenic • Non-accidental injury • Cessation of smoking may aggravate ulceration
Diagnosis • Based on history and clinical features • To exclude underlying systemic conditions diagnostic testing as follows is required: Full Blood count, Haematinics – ferritin, folate, vitamin B12 Serological test for coeliac disease - tissue transglutaminase antibody or antiendomysial antibody • Clinical Features: site,size, shape, number of ulcers in crop, frequency & duration of episodes, age of onset, any systemic features? • Tissue biopsy if SCC suspected
Management & Treatment First Line Therapies • Good OH • Dispersible Doxycycline (100mg) & CHX mouthwashes • Topical Analgesics – 0.15% Benzydamine Hydrochloride (Difflam) or 1% Lidocaine ointment • Mucosal protectants – carboxymethylcellulose (orobase) • Topical Corticosteroids (on prescription) – 2.5mg Hydrocortisone muco-adhesive buccal tablet, 0.5mg soluble betamethasone phosphate tablets (mouthwash) or BeclometasoneDipropionate Spray Fluticasone propionate spray, mouthwash or ointment (off prescription)
Second Line Therapies • Systemic corticosteroid/immunosuppressive treatment for severe cases • Azathioprine • Clofazimine • Colchicine *Only under consultant-led treatment*
Referral of Suspicious Lesions When to Refer?? • Single ulcers persisting for longer than 3 weeks • Ulcers with an indurated border • Ulceration unresponsive to topical therapy • ROU of uncertain aetiology • RAS impacting on an individuals quality of life • Suspected SCC – URGENT referral
References • ORAL ULCERATION: AN OVERVIEW OF DIAGNOSIS AND MANAGEMENT PRIYA THAKRAR, SHAHID I CHAUDHRY Prim Dent J. 2016;5(1):30-33 • Oral Medicine: 1. Ulcers: Aphthous and other Common Ulcers David H Felix, Jane Luker, Crispian Scully Dental Update 2012; 513-519