Download
1 / 26
260 likes | 504 Views
C oarctation of the Aorta. Liz Wetzel, MD CICU Rounds November 19, 2010. Objectives. Review Anatomy/Lesion Development Discuss DR Presentation and Management Review Post-natal Evaluation and Transport

E N D
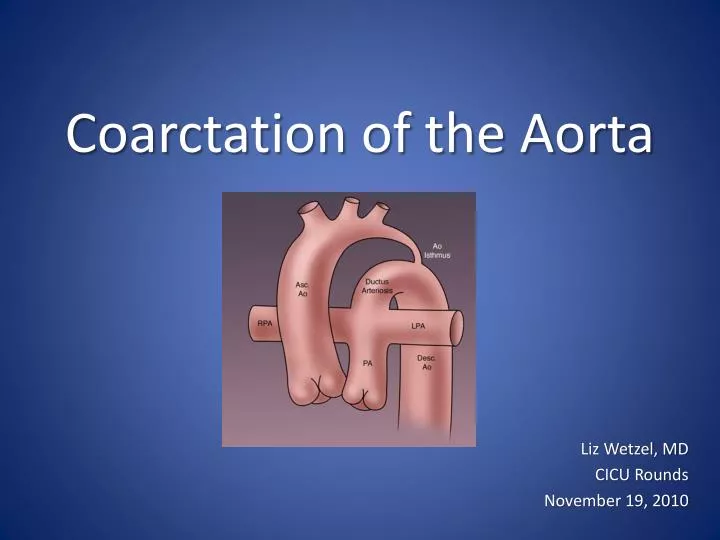
Coarctation of the Aorta Liz Wetzel, MD CICU Rounds November 19, 2010
Objectives • Review Anatomy/Lesion Development • Discuss DR Presentation and Management • Review Post-natal Evaluation and Transport • Describe possible presentation in non-prenatally diagnosed cases and timing of duct closure • Discuss potential CICU Course and outcomes
Development of the aortic arch The left fourth arch vessel becomes the arch of the aorta. The left 6th becomes part of the left pulmonary artery and the ductus arteriosis. Sadler, TW. Langman’s Medical Embryology 8th edition. Philadelphia: Lippincott Williams& Wilkins,2000: 239-243.
Development continued Molin, D. DeRuiter, M.C, Wisse, L.J, Azhar, M., Doetschman, T., Poelmann, R. E., Gittenberger-de Groot, A. C. Altered apoptosis pattern during pharyngeal arch artery remodeling is associated with aortic arch malformations in Tgfβ2 knock-out mice. Cardiovascular Research. 2002; 56: 312-322. Gittenberger-De Groot, A.C. Bartelings, M.M. Deruiter, M.C. Poelmann, R.E. Basics of Cardiac Development for the Understanding of Congenital Heart Malformations. Pediatric Research. 2005; 57 (2): 169-176.
Development of Coarctation • Abnormal development of left 4th and 6th aortic arches • Represents 5-10% of all congenital cardiac lesions • More common in boys than girls • No real impact prior to birth due to presence of PDA unless there is fetal closure
Ductus Tissue Theory Hemodynamic Theory Reduced intrauterine blood flow causes underdevelopment of aortic arch Results from reduced volume of blood flow through the fetal aortic arch and isthmus • Due to a migration of ductus smooth muscle cells into the periductal aorta with subsequent constriction and narrowing of the aortic lumen • Evident when ductus closes
Other Theories • May be due to a defect in the vascular wall of the ascending aorta • Vascular apoptosis may have a role (Molin et al 2002) • Recessive genetic mutation found in zebrafish (Weinstein et al 1995) • Autosomal dominant inheritance of non-syndromic left ventricular outflow tract obstruction (Wessels et al 2005)
DR Presentation & Management • Follow normal NRP guidelines for resuscitation and be sure to have a stable airway • This is not a lesion where you would expect acute delivery room decompensation • Should not be a blue baby due to the heart defect • Admit to the NICU
Management in the NICU • Support the airway (intubation if necessary) • Echocardiogram and CXR • Ideally establish umbilical access • PGE1 infusion (0.03 to 0.05 mcg/kg/min) • Correct acidosis and electrolyte abnormalities • Blood pressure support as indicated • Main goal is to stabilize the patient and get them transferred to a cardiac intensive care unit
Transport Issues and Hand-off to cards • Be confident you have a stable airway • Risk of apnea with PGE1 infusion, consider caffeine? • Have secure IV access with fluids running • PGE1 infusion can cause vasodilatation and can result in relative hypovolemia in neonates • Report recent blood gas with electrolytes including ionized calcium and potentially a lactate • Full set of vitals including 4 extremity blood pressures
Undiagnosed Coarctation Presentation • Decreased or absent femoral pulses, tachypnea, grunting, poor feeding, signs of CHF, abnormal 4 extremity blood pressures • If coming from home can present to ED in shock with multi-organ dysfunction and severe metabolic acidosis • CXR with cardiomegaly, pulmonary congestion Sharland, G.K, Chan, KY, Allen, LD. Coarctation of the aorta: difficulties in prenatal diagnosis. British Heart Journal. 1994; 71: 70-75. http://www.heartonline.org/congenital.htm
Potential CXR Progression DAY THREE OF LIFE DAY FIVE OF LIFE
Closure of the duct • Functional and Anatomic Closure of Duct • Closure occurs in three steps: • constriction of ductal smooth muscle; • hypoxia/ischemia of medial smooth muscle; • remodeling resulting in permanent closure (Koch et. al 2006) • In term infants functional closure can occur as early as 12-15hours of age, if greater than 72 hours it is considered persistent, trueanatomicclosure can take weeks Neoreviews Controversies in the Management of PDA (Gien 2008)
Timing of Ductal Closure • In >95% of neonates >1500g closure usually begins within 96 hours (Koch et. al 2006) • Spontaneous closure occurs in >34% of ELBW neonates (Koch et. al 2006)
Potential surgical intervention • First surgery was done experimentally in animals in 1944 – Blalock and Park • 1. Resection with end-to-end anastomosis • 2. Patch aortoplasty • 3. Left subclavian patch aortoplasty • 4. Bypass grafts between ascending and descending aorta Rothman, Abraham. Coarctation of the Aorta: An Update. Current Problems in Pediatrics. 1998; 37-60.
Cincinnati Children’s Experience • Preferred approach here is end-to-end anastomosis • Most important determinant of outcome is how fast it is detected and how soon they head to the OR • Typically in the OR within 12 hours of admission to CICU • Usual length of stay is 2 days in CICU and a total of 5 days in the hospital (unless very sick prior to OR) • Less than 5% need re-intervention Courtesy of Dr. Angela Lorts; Cardiac Critical Care Staff; Cincinnati Children’s Heart Institute
Surgical outcomes • Acute mortality ranged from 3% to 32%, strongly correlated with complexity of associated cardiovascular lesions • Lowest in those with isolated coarcation (<2%) • Restenosis rate was 3-41% Rothman, Abraham. Coarctation of the Aorta: An Update. Current Problems in Pediatrics. 1998; 37-60.
Survival Data • Quaegegbeur et al. reported on a multi-institutional study that looked at 326 severely symptomatic neonates with coarctation and with or without VSD. • The 1 month survival was 93% and the 24 month survival was 84%. Quaegebeur, J.M, Jonas, R.A, Weinberg, A.D, Blackstone, E.H, Kirklin, J.W. Outcomes in seriously ill neonates with coarctation of the aorta, A multiinstitutional study. The Journal of Thoracic and Cardiovascular Surgery. 1994; 108: 841-854.
Post-operative complications • Hoarseness • Ipsilateral diaphragm paralysis • Chylothorax • Vessel injury/bleeding • Rebound HTN • Post-coartectomy syndrome • Paralysis due to spinal cord ischemia
Long term complications • Re-stenosis: influenced by presence of residual ductal tissue within the aorta • Hypertension: more likely in repair at a later age • Neurologic abnormalities • Ultrasound abnormalities • microcephaly
Neurologic abnormalities Preoperative neurobehavioral abnormalities: abnormal tone, posturing, weak cry, poor suck, poor auditory and visual orienting Abnormal ultrasound findings: ventriculomegaly, IVH, basal ganglia calcification, widened subarachnoid spaces found preoperatively Limperopoulos C, Majnemer A, Shevell M, Rosenblatt, Rohlicek C, Tchervenkov C. Neurologic Status of Newborns With Congenital Heart Defects Before Open Heart Surgery.Pediatrics. 1999; 103(2): 402-408.
THANK YOU TO MY ADVISOR DR. KRAWCZESKI ANY QUESTIONS?????
References • Brouwer, R.M, Erasmsus, M.E, Ebels, T, Eijgelaar, A. Influence of age on sruvival, late hypertension, and recoarctation in elective aortic coarctation repair: Including long-term results after elective aortic coarctation repair with a follow-up from 25 to 44 years. The Journal of Thoracic and Cardiovascular Surgery. 1994; 108: 525-531. • Chang RK, Gurvitz M, rodriguez S. Missed Diagnosis of Critical Congenital Heart Disease. Arch PediatrAdolesc Med. 2008; 162(10): 969-974.. • De-Wahl Granelli, A, Mellander M, Sunnegardh J, Sandberg K, Ostman-Smith I. Screening for duct-dependent congential heart diseaswe with pulse oximetry: A critical evaluation of strategies to maximize sensitivity. ActaPediatrica. 2005;94: 1590-1596 • Gittenberger-De Groot, A.C. Bartelings, M.M. Deruiter, M.C. Poelmann, R.E. Basics of Cardiac Development for the Understanding of Congenital Heart Malformations. Pediatric Research. 2005; 57 (2): 169-176. • Johnson BA and Ades A. Delivery Room and Early Postnatal Management of Neonates Who Have Prenatally Diagnosed Congenital Heart Disease. Clinics in Perinatology. 2005; 32: 921-946. • Limperopoulos C, Majnemer A, Shevell M, Rosenblatt, Rohlicek C, Tchervenkov C. Neurologic Status of Newborns With Congential Heart Defects Before Open Heart Surgery.Pediatrics. 1999; 103(2): 402-408. • Molin, D. DeRuiter, M.C, Wisse, L.J, Azhar, M., Doetschman, T., Poelmann, R. E., Gittenberger-de Groot, A. C. Altered apoptosis pattern during pharyngeal arch artery remodelling is associated with aortic arch malformations in Tgfβ2 knock-out mice. Cardiovascular Research. 2002; 56: 312-322. • Polin,Fox,Abman. Fetal and Neonatal Physiology 3rd edition. Mechanisms Regulating Closure of the Ductus Arteriosis. Saunders. Pennsylvania 2004: 743-747. • Quaegebeur, J.M, Jonas, RShultz A, Localio A, Clark B, Ravishankar C, Videon N, Kimmel S. Epidemiadnologic Features of the Presentation of Critical Congenital Heart Disease: Implications for Screening. Pediatrics. 2008;121(4) 751-757. • .A, Weinberg, A.D, Blackstone, E.H, Kirklin, J.W. Outcomes in seriously ill neonates with coarctation of the aorta, A multiinstitutional study. The Journal of Thoracic and Cardiovascular Surgery. 1994; 108: 841-854. • Rothman, Abraham. Coarctation of the Aorta: An Update. Current Problems in Pediatrics. 1998; 37-60.
References • Sadler, TW. Langman’s Medical Embryology 8th edition. Philedelphia: Lippincott Williams& Wilkins,2000: 239-243. • Sharland, G.K, Chan, KY, Allen, LD. Coarctation of the aorta: difficulties in prenatal diagnosis. British Heart Journal. 1994; 71: 70-75. • Weinstein, BM, Stemple, DL, Dreiver W, Fishman, MC. Gridlock, a localized heritable vascular patterning defect in the zebrafish. Nat Med. Nov 1995; 1(11): 1143-1147. • Wessels, M.W, Berger, R, Frohn-Mulder, I, Roos-Hesselink, J.W, Hoogeboom, J, Mancini, G.S, Bartelings, M.M, De Krijger, R, Wladimiroff, J.W, Niermeijer, M.F, Grossfeld, P, Willems, P.J. Autosomal Dominant Inheritance of Left Ventricular Outflow Tract Obstruction. American Journal of Medical Genetics. 2005; 134A: 171-179. • Zehr K, Gillinov M, Redmond M, Greene PS, Kan J, Gardner TJ, Reitz B, Cameron D. Repair of Coarctation of the Aorta in Neonates and Infants: A Thirty-Year Experience. Annals of Thoracic Surgery. 1995; 59: 33-41. • http://www.heartonline.org/congenital.htm • Title page image: www.odlarmad.com
Survival Data based on Age Brouwer, R.M, Erasmsus, M.E, Ebels, T, Eijgelaar, A. Influence of age on sruvival, late hypertension, and recoarctation in elective aortic coarctation repair: Including long-term results after elective aortic coarctation repair with a follow-up from 25 to 44 years. The Journal of Thoracic and Cardiovascular Surgery. 1994; 108: 525-531.