Download
1 / 12
180 likes | 491 Views
The immune response against Mycobacterium tuberculosis. MBChB II Respiratory System. MTB infection and disease. 1/3 of world population is infected (infection does not equal disease) Latent MTB infection (LTBI), dormant bacilli Huge reservoir for future disease

E N D
The immune response against Mycobacterium tuberculosis MBChB II Respiratory System
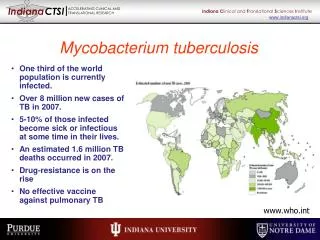
MTB infection and disease • 1/3 of world population is infected (infection does not equal disease) • Latent MTB infection (LTBI), dormant bacilli • Huge reservoir for future disease • Active infection= ‘tuberculosis’ (>9M new cases/year, leading cause of death due to bacterial infection, ±3M deaths /year) • Interplay between HIV and MTB • Multi-drug resistant (MDR) or Extensive drug resistant (XDR) strains on the increase
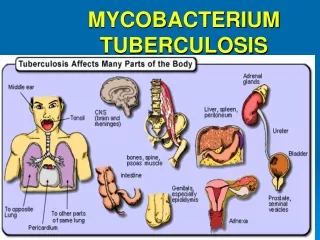
MTB transmission • Spread by inhalation of small droplet nuclei which are aerosolized infectious particles generated by coughing, talking or sneezing • Particles remain airborne for long periods • When inhaled, particles are deposited in the terminal airways where viable bacilli can cause infection. A single cough can generate up to 3000 infectious droplets and sneezing many more • Large respiratory droplets and fomites are not important sources of MTB transmission • Transmission most commonly occurs indoors in the setting of prolonged exposure and multiple inocula. The risk of infection is determined by the closeness of the contact (often household or institutional) as well as the infectiousness of the source case (more in smear positive cases, people with lung cavities if HIV negative. In HIV positives transmission occurs also without cavities)
MTB Infection and TB disease • Not all exposed people become infected (approx 1/3) • Not all transmission leads to persistent infection • Only 3-5% of infected people become diseased within 12 months and 5-15% in their lifetime • Impaired immunity may lead to TB disease: host genetic factors (i.e. IFNγ receptor deficiency), HIV/AIDS, malnutrition, alcoholism, renal failure, immunosuppressive therapy and diabetes mellitus
The stages of latent infection to disease • Latent infection is asymptomatic and is identified based on the presence of a T-cell response directed against mycobacterialantigens (positive tuberculin skin test (TST) or interferon gamma release assay (IGRA)) (see later). • Clinical classification of MTB infection as being either latent or active is an oversimplification • MTB infection can be classified according to four response spectra based on the host immune reaction to the organism • Innate immune stage: the host innate immune response is able to eradicate the infection without the need for acquired immune responses and with a subsequent absence of detectable immunological memory against the organism. • Acquired immune stage: both the innate and acquired immune systems operate to eliminate the infection. • Quiescent infection stage: the host immune system can still control the infection although there are viable (but non-replicating) organisms. • Active infection stage: bacteria are not only viable but able to replicate. At this stage, the host immune response is still able to control the infection up to the point where there are no symptoms or signs of infection. Progression of the infection beyond this point will lead to clinically apparent infection or active disease.
Immune Diagnosis of MTB infection Delayed type hypersensitivity • Tuberculin skin test, Mantoux test, PPD test • Also multiple puncture tests like Tine, Heaf tests The stages of a delayed type hypersensitivity reaction.
Figure 12-25 New tests for MTB infection: interferon gamma release assays= IGRA’s • Overnight culture of either whole blood (Quantiferon) or peripheral blood mononuclear cells (PBMC’s) (T-Spot.TB) in the presence of MTB specific antigens • Rely on pre-existing memory T cells against MTB antigens • Probably more specific that TST • As sensitive as TST • More expensive than TST (>10 US$) • Requires lab expertise • More standardized that TST • Require only one visit to health care worker (i.e. can phone result through) • Not enough data on performance in high incidence settings, in children and in HIV infection Quantiferon test T-Spot.TB test
Pathogenesis: innate immune cells induce T cells Infected alveolar macrophages or interstitial dendritic cells (DCs) migrate to draining lymph nodes and stimulate antigen-specific T cells. The lung lesion plus these lymph nodes form the Ghon complex. APC’s activate T cells Or Infected macrophages and DCs enter the lung parenchyma and attract monocytes from the blood. Mononuclear phagocytes form a granuloma but are orchestrated by T cells. Granuloma: surrounded by a fibrotic wall, separated from the surrounding tissue and its center becomes necrotic. MTB is now contained and dormant, unable to cause disease until the host is weakened.
…Pathogenesis: the bug shuts down its metabolism, temporarily… -In the granuloma: hypoxic conditions. MTB switches its gene expression from highly active, replicative to dormancy (DosRregulon). No growth, reduced respiration and metabolism. Become non-stainable by conventional methods like ZiehlNeelsen acid fast stain. -Once the lesion is disrupted: MTB synthesizes RNA and DNA, divide, become resuscitated. May be due to resuscitation promoting factor s (RPF’s) secreted by a few metabolically active bugs- act as pheromones for dormant bacteria. These rpf’s are enzymes that dissolve cell walls. -MTB then flourishes in liquefied lesion and is transmitted through blood stream or airways to other parts of the body. Multiple caseatinggranulomas in the lung
Multiple ways to subvert macrophage function during MTB infection Interference with phagosome-lysosome fusion Prevention of phago-lysosome acidification Decreased induction by IFN-gamma Down-regulation and degradation of MHC class II Lack of upregulation of co-stimulatory molecules
So what goes wrong with the adaptive immune system in TB? Loss of immune memory MTB changes antigens: Memory T cells become effector T cells when they encounter antigen. MTB has 4000 genes and may stop expressing antigens that were expressed during early infection. Effector cells that are generated during early infection keep things in check but are not as long lived as memory cells and decrease over time. The memory cells that are specific for early infection antigens become less useful as MTB now uses different antigens. Exhaustion of memory: persistent antigen coupled with strong stimulation also leads to loss of memory cells.
So what goes wrong with the adaptive immune system in TB? Wrong T cell phenotypes -Th1 cells are needed (produce IFNγ, TNFα, IL-12 etc) for effective control of MTB infection. -Th2 cells(produce IL4, IL5, IL-10, IL-13, etc) and regulatory T cells (produce IL-10, TGFβ) prevent immunopathology but also suppress Th1 cells and if this balance is disturbed MTB may escape immune control.