Download
1 / 24
240 likes | 380 Views
Session #F4 - 20 October 29, 2011 10:50 AM. A Dementia Case‐Finding Program for Veterans: Applying Lessons Learned to Improve Dementia Recognition in Primary Care Practice. Laura O. Wray, PhD, Director of Education, VA Center for Integrated Healthcare

E N D
Session #F4 - 20 October 29, 201110:50 AM A Dementia Case‐Finding Program for Veterans: ApplyingLessons Learned to Improve Dementia Recognition in Primary CarePractice Laura O. Wray, PhD, Director of Education, VA Center for Integrated Healthcare David A. Hunsinger, MD, MSHA, Medical Director, Binghamton VA Outpatient Clinic Collaborative Family Healthcare Association 13th Annual Conference October 27-29, 2011 Philadelphia, Pennsylvania U.S.A.
Faculty Disclosure We have not had any relevant financial relationships during the past 12 months.
Need/Practice Gap & Supporting Resources • Costs of care for patients with dementia are significantly greater than costs for similarly aged • Significant impairment in medical adherence can occur long before dementia is recognized • Rates of detection of dementia in primary care are low • Undiagnosed dementia is a missed opportunity to improve quality of care and quality of life for our older patients • First step in improving care is to increase recognition
Objectives • Describe the experience of VA Upstate New York Veteran’s Integrated Health Care System (VISN 2) in using an electronic medical record based system to identify Veterans to be screened for dementia • Review guidelines for recognition of dementia • Discuss how medical and behavioral health providers can work collaboratively to address this challenge
Expected Outcome Attendees will be able to discuss how common risk factors can be used to improve the detection of dementia in primary care
Dementia Recognition in Primary Care (PC) • USPSTF: “Insufficient evidence to recommend foror against screening” • 25-40% cases recognized: typically when moderately impaired • What delays dementia diagnosis?` • Provider • Time constraints • Absence of family informant • Provider attitudes: Dementia is untreatable • Patient • Agnosagnosia • Acceptability of screening • Family discomfort with raising concerns
Highlights of American Academy of Neurology Guidelines • Know and Share the 10 Warning Signs • Be alert to cognitive impairment • Know and use a brief mental status measure (example: Mini-Cog Borson S, et al. Int J Geriatr Psychiatry. 2000; 15: 1021-1027.) • Clinical Criteria for AD are reliable • Include routine evaluation of: • CBC • Glucose • Depression Screening • Thyroid Function • Serum electolytes • BUN/creatine • Serum B12 • Liver function
Ten Warning Signs of AD • Memory loss that affects job skills • Difficulty with familiar tasks • Problems with language • Disorientation to time and place • Poor or decreased judgment • Problems with abstract thinking • Misplacing things • Changes in mood or behavior • Changes in personality • Loss of initiative
VISN 2 RAPID* Goals: • Promote early recognition of cognitive impairment and diagnosis of dementia • Provide access to comprehensive assessment for Veterans who screen positive for cognitive assessment • Offer education and support to caregivers • Provide access to dementia care management *RAPID = Recognizing and Assessing Progression of cognitive Impairment and Dementia
VISN 2 RAPID Program Overview Clinical Reminder used to generate monthly RAPID eligible list Behavioral Health Assessment Center (BHAC)* +/- + Dementia Care Coordinator +/- Primary Care Provider + Geriatric Evaluation & Management (GEM) + +/-
RAPID Case Finding Approach:Use of Dementia Red Flags • Electronic Medical Record: • Age (Over 70)* • And one or more of the following: • 2 or More ER visits in past year • History of CVA • Taking more than 1 anticholinergic medication • Behavioral Health Assessment Center (BHAC) performs cognitive screen • Dementia Care Manager calls veteran and family informant and reviews medical record • Medication adherence problems • More than 7 prescribed medications • Agitation • Multiple falls in past year • More than 2 hospitalizations • Attending office visit with caregiver • More than 2 missed appointments in past year • DX of Diabetes + hypertension + CAD + hyperlipidemia Adapted from the work of Callahan, Boustani, Unverzagt et al., Ann of Int Med (2006)
RAPID Screening Calls • Monthly call lists – clinical reminder technology • Adaptable to adjust # of patients to be screened • Blessed Orientation Memory and Concentration Test (BOMC) • Validated for use over the phone • Routinely used as part of BHL software • New introduction script created • Score = Total Errors; Range = 0 - 28 • ≥10 is suggestive of dementia
RAPID Case-Finding Strategy • Call List Criteria • Primary Care appointment within the coming month • No prior dementia diagnosis • Veterans 70* years and older And Either • One or more anticholinergic medication OR • History of CVA OR • Two or more ER visits in last year • BHAC calls veteran • Positive BOMC (11 or greater) referred to DCM • Negative BOMC healthy brain questions and feedback about preserving memory via lifestyle
Program Evaluation Methods - Sample • All VISN 2 Veterans aged 70 and over • At least 1 appointment at any VISN 2 medical center primary care FY07 - FY09 • Exclusions: • Diagnosis of dementia in FY05 – FY07 • Prescription for Cholinesterase Inhibitor of NMDA receptor antagonist • Missing any data for any risk factor • Example: PHQ-2 (2,881 Veterans)
Program Evaluation Methods - Sample • Sample Categorization • RAPID Eligible Veterans • 70 yrs and older and any of the following: • 2 or more ER Visits • History of CVA • 1 or more anticholinergic medications • Within RAPID Eligible: • BOMC + Veterans: Score 10 or greater • BOMC – Veterans: Score of less than 10 • Unscreened Veterans: no evidence of a RAPID screening call in EMR
Program Evaluation Methods • Index Date: to track time to diagnosis • Unscreened Group: first medical appointment after 10/1/07 • Screened Group: date of the RAPID call • Incidence of New Dementia Diagnosis • 1st occurrence of visit encounter coded for dementia following Index Date
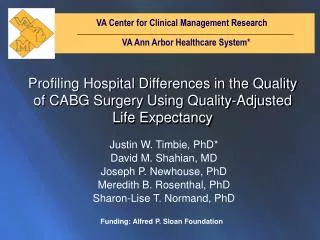
Within RAPID Eligible Veterans, is a BOMC+ associated with a new dementia diagnosis? Incidence of Dementia among RAPID Screen Positive Veterans
Within RAPID Eligible Veterans, is a BOMC+ associated with a new dementia diagnosis? HR = 4.97 (95%CI: 2.32 –10.66)
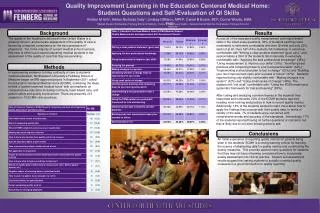
Which Risk Factors Predict Dementia Diagnosis? • EMR Risk Factors: • Age • Gender • ER Visits • Diabetes • Hypertension • Head Trauma • CVA • TIA • Health Screens for: • Tobacco • Alcohol Use (Audit-C) • Depression (PHQ-2)
What are EMR risk factors are most effective identifying dementia? Risk Model for Incidence of New Dementia Diagnosis
Summary • Age, ER use, and History of CVA continue to be strong risk factors. • Depression is also an important predictor • Older adults with PHQ+ or in MH treatment should be considered for dementia screening • Program activities following a BOMC+ associated with a 5x increase in new dx • Supporting identification of dementia can improve PC recognition rates
Questions for the presenters? Group Discussion: How can the detection of dementia be improved in primary care?
Session Evaluation Please complete and return theevaluation form to the classroom monitor before leaving this session. Thank you!