Download
1 / 33
330 likes | 601 Views
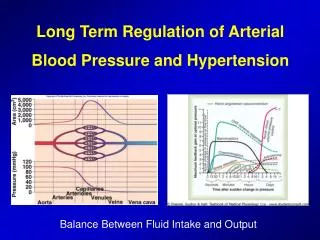
Regulation of blood pressure. & Special circulations. Long-term and short-term control of ABP. Short-term. Baroreflex. heart. resistence & comp liance. Blood Volume. Long-term. hypertrophy. Angiotensin II Vasopressin NO ANP Endothelin Sympathetic nervous system. drinking

E N D
Regulation of blood pressure & Special circulations
Long-term and short-term control of ABP Short-term Baroreflex heart resistence & compliance Blood Volume Long-term hypertrophy Angiotensin II Vasopressin NO ANP Endothelin Sympathetic nervous system drinking renal excretion Na-intake Ackermann
Myogenic autoregulation • Arterioles contracts when they are distended (brain, kidney, heart) • Mechanism • Stretch-activated Na+ and Ca2+ channels of vascular smooth muscle • Depolarization of membrane, which then activates L-type Ca2+ channels • Muscle contraction
Metabolic regulation • Adenosine • Causes vasodilatation, except of kidney and pulmonary artery • Activation of adenosine A2A membrane receptor – elevation of cAMP • pO2 • Reduction in pO2increases production of vasodilator agents (PGI2 and NO) • pCO2 • Elevated pCO2 leads to elevated H+ in extracellular fluid – acidosis causes membrane hyperpolarization (K+) – vasodilatation (except of lung)
Shear-dependent regulation • Endothelial cell reacts on many physiological stimuli with production of several substances which influence smooth muscle cell • Stretching • Shear stress induced by blood flow • Hormonal levels • Substances released from blood elements (trombocytes, macrofages) • Synthesis of NO and PGI2 (vasodilators)
Nitric oxide synthesis • Shear stress and a variety of receptor-mediated agonists raise vascular endothelial [Ca++] and cause the Ca++-calmodulin complex to activate endothelial nitric oxide synthase (eNOS). • NO is produced from the amino acid L-arginine. • NO is a gas and diffuses into adjacent VSM where it activates soluble guanylate cyclase, produces cGMP and causes vasodilatation Ackermann
Neural regulation • Sympathetic nerves • Constrictor nerves – mediator noradrenaline - a1 adrenoreceptors • Elevates Ca++ through phospholipase C pathway (IP3) • Parasympathetic nerves • In tissues which need sudden increase in blood flow (salivary gland, external genitalia) • Mediator acetylcholine has indirect effect • inhibition of noradrenalin release • production of NO
Hormonal regulation • Renin-angiotensin, vasopressin, ANP • Adrenaline (epinephrine) • Higher affinity for b-adrenoreceptors (heart, splanchnic area, skeletal muscle) – vasodilatation • Lesser affinity for a-adrenoreceptors (vasoconstriction) • Serotonin • released from platelets during clotting reaction, elevated Ca2+ leads to vasoconstriction • Histamine • Vasodilatation by means of NO production
Renin-angiotensin II-aldosteron system • Regulates ABP by regulating blood volume • A decrease in ABP – decrease in renal perfusion pressure • Mechanoreceptors in afferent arterioles • Juxtaglomerular cells secret renin (proteolytic enzyme) • In plazma, renin catalyzes the conversion of angiotensinogen to angiotensin I (a decapeptide) • In lungs, angiotensin I is converted to angiotensin II (catalyzed by angiotensin converting enzyme (ACE) (an octapeptide)
Role of angiotensin II • In the zona glomerulosa cells of adrenal cortex stimulates production of aldosterone • In renal distal tubule and collecting duct increases Na+ reabsorption – increases ECF volume and blood volume • In arterioles angiotensin II causes vasoconstriction – increase in TPR • In the renal proximal tubule stimulates Na+-H+ exchange – increase in ECF volume • In the CNS stimulates thirst an drinking behavior
Antidiuretic hormone • Secreted by the posterior lobe of the pitiutary gland after • increased osmolarity • decreased ABP (e.g. hemorrhage), atrial volume receptors are stimulated • Regulates body fluid osmolarity • 2 types of receptors: • V1: in vascular smooth muscles – cause vasoconstriction of arterioles, increase TRP • V2: in renal collecting ducts are involved in water reabsorption, maintain osmolarity
Atrial natriuretic peptide • ANP is secreted by the atria in response to increase in ECF volume and atrial pressure • Mechanism of action: • Relaxation of vascular smooth muscle – vasodilatation, decrease TPR • In the kidney – increased Na+ and water excretion = decrease ECFV and ABP
Chemoreceptors in carotid and aorctic bodies • Chemoreceptors – high rates of O2 consumption, sensitive to decrease of pO2 • Afferentatiton to the medullary cardiovascular centers – increase in sympathetic outflow to the heart and blood vessels – increase ABP and delivery of O2 • Chemoreceptors are also sensitive to pCO2 and pH, but the reflexes are smaller compared with changes in pO2
Cerebral chemoreceptors • Chemoreceptors in the medulla are most sensitive to pCO2and pH and less sensitive to pO2 • Reflex during decreased cerebral blood flow: • increase in pCO2and decrease in pH activates chemoreceptors • Increase in both sympathetic and parasympathetic outflow • Increased contractility, increased TPR but decreased heart rate • Intense arteriolar vasoconstriction redirects blood flow to the brain
Baroreceptors • Baroreceptors are mechanoreceptors – sensitive to changes in pressure or stretch • located within the walls of the carotid sinus and the aorctic arch • Carotid sinus – (changes in arterial pressure) - afferent IX. cranial nerve n. glossopharyngeus • Aorctic arch – (increase in arterial pressure) X. cranial nerve n. vagus • cardiovascular vasomotor centers in the brain stem • Baroreflex - fast regulation – via changes in he output of sympathetic and parasympathetic NS
Brain stem cardiovascular centers • Localized in reticular formation of medulla and lower 1/3 of the pons • Information from IX. and X. nerves is integrated in nucleus tractus solitarius and redirected to • Cardiac decelerator center – PNS – n. vagus – SA node – decrease heart rate • Cardiac accelerator center – SNS – SA node (increase heart rate, conduction velocitythrough the AV node, contractility) • Vasoconstrictor center – SNS – vasoconstriction of arterioles and venules
Midbrain regions of CV control Area postrema Rostral ventrolateral medulla Cardiac accelerator center Vasoconstrictor center Nucleus tractus solitarius Nucleus ambiguous Cardiac decelerator center Caudal ventrolateral Medulla Fibers from this neurons project to the vasoconstrictor area and inhibit it
Sympathetic nerveactivityand arterial pressure • Decreasing blood pressure is followed with increasing sympathetic nerveactivity • Vasoconstriction increases blood pressure
Regulation of mean arterial pressure (ABP) ABP (mmHg) = cardiac output (ml/min) x total peripheral resistance (mmHg/ml/min) CO = stroke volume (ml) x heart rate (c/min) • Cardiac output and TPR are not independent variables • when TRP increases, CO compensatory decreases • Regulation of ABP – comparing ABP with the set-point value (100 mm Hg)
increased activity of NA decreased activity CAC decreased activity VC activation of baroreceptors increase firing rate in IX., X. increase in ABP cardiac decelerator center decrease of heart rate increased parasymp. outflow stimulation of NTS decrease of heart rate contractility decreased sympathetic outflow vasodilatation CAC - cardiac accelerator center, VC – vasoconstrictor center
Estimation of baroreceptor sensitivity Index of baroreceptor sensitivity = PI/SBP (ms/mmHg)
Association between broreceptor sensitivity and hypercholesterolemia Persons with higher level of LDL cholesterol have lower baroreceptor sensitivity Koskinen et al. 1995
Changes in posture from supine position to standing • Mechanism of orthostatic hypotension • Blood pools in the veins of lower extremities • Venous return to the heart decreases, cardiac output decreases (Frank-Starling law) • Mean arterial pressure decreases • Decreased activation of baroreceptors • Increased sympathetic outflow to the heart and blood vessels and decreased parasympathetic outflow
Special circulations • Different organs have • Differences in vascular resistance • Differences in metabolic demands • Local control (intrinsic) • Hormonal control (extrinsic)
Cerebral circulation • 15 % of cardiac output • Is controlled by local metabolites • pCO2(H+) is the most important vasodilator • CO2 diffuses to vascular cells, forms H2CO3 (H+) • Intracellular H+causes vasodilatation • Increase in blood flow, removal of excess CO2 • Decrease in pO2 increases cerebral blood flow • Many vasoactive substances do not affect cerebral circulation, do not cross the blood-brain barrier
Coronary circulation • 5 % of cardiac output • Local metabolic factors • Hypoxia: increase in myocardial contractility – increased O2 consumption – local hypoxia • Hypoxia causes vasodilatation of the coronary arterioles – compensatory increase in blood flow and O2 delivery • Adenosine (from ATP) causes vasodilatation • Mechanical compression of the blood vessels during systole in the cardiac cycle – brief period of occlusion and reduction of blood flow
Pulmonary circulation • 100% of cardiac output • Lower pressure and low resistance • Controlled by local metabolites, primarily by pO2 (bellow 70 mm Hg) • Opposite effect than in other tissue – hypoxia causes vasoconstriction • Mechanism – inhibition of NO production in endothelial cells of blood vessel walls • Redistribution of blood from poorly ventilated areas to well-ventilated areas
Renal circulation • 25 % of cardiac output • Renal blood flow is autoregulated • Constant blood flow even when renal perfusion pressure changes (80-200 mmHg) • Renal autoregulation is independent of sympathetic innervation (transplanted kidney) • Angiotensin II – vasoconstrictor for both afferent and efferent arterioles, but efferent arteriole is more sensitive • Prostaglandins (E2, I2 – produced locally) – vasodilatation of both arterioles
Skeletal muscle circulation • 25 % of cardiac output • Sympathetic innervation • At rest: activation of a1 (noradrenaline) receptors causes vasoconstriction, increased resistance and decreased blood flow • Activation of b2 (adrenaline) receptors causes vasodilatation • Local metabolites • During exercise: local vasodilator – lactate, adenosine, K+
Skin circulation • 5 % of cardiac output • Dense sympathetic innervation – regulates blood flow for regulation of body temperature • Increase core body temperature – decrease sympathetic tone to the smooth muscle sphincters controlling A-V anastomoses - increase skin blood flow • Arteriovenous anastomoses – permit bypass of the capillary vessels