Download
1 / 28
300 likes | 716 Views
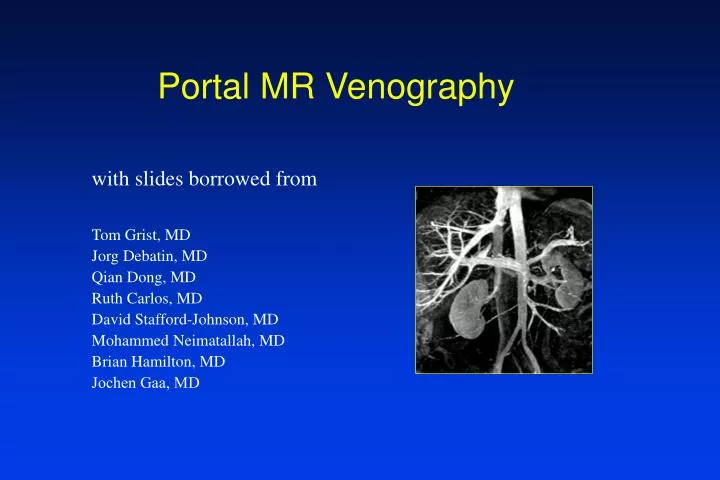
Portal MR Venography . with slides borrowed from. Tom Grist, MD Jorg Debatin, MD Qian Dong, MD Ruth Carlos, MD David Stafford-Johnson, MD Mohammed Neimatallah, MD Brian Hamilton, MD Jochen Gaa, MD. Portal venous phase. Arterial phase. Coronal 3D Gd MRA of Portal Vein. Coronal Plane

E N D
Portal MR Venography with slides borrowed from Tom Grist, MD Jorg Debatin, MD Qian Dong, MD Ruth Carlos, MD David Stafford-Johnson, MD Mohammed Neimatallah, MD Brian Hamilton, MD Jochen Gaa, MD
Portal venous phase Arterial phase
Coronal 3D Gd MRA of Portal Vein • Coronal Plane • Field of view = width of patient (28-32 cm) • Thick slices: 3-5 mm • Zero padding • Fast enough for breath holding • TR < 10 msec • TE < 3 msec • Partial Fourier imaging (0.5 NEX) • Adjust phase encoding steps (128-224) • Three phases • Arterial • Portal venous • Equilibrium
Mesenteric Portal Protocol • Sequence Time • Sag SSFSE 0:56 • Axial T1 5:32 • Axial T2 & fat sat 6:04 • MRCP (optional) • Coronal 3D Gd (3 phases) 0:30 x 3 • Axial 2D TOF (optional) • Total imaging time ~15-25 minutes
Arterial Phase Venous Phase
Hepatoma Venous Phase
Fig. 7.7. Hepatoma. Clinical Scenario: 54-year-old female with abdominal pain and elevated AFP. Technique: Coronal Acquisition, TR/TE/Flip = 8.1/2.1/45°, Field-of-View = 320 x 320 x 96 mm, Matrix 256 x 160 x 32, Centric Ordering of k-space, Acquisition Time = 29 s, 40 ml gadolinium contrast infused at 2 ml/s, and timed empirically. Interpretation: A coronal MIP from the portal venous-phase of the contrast bolus shows an enhancing mass in the dome of the liver with heterogenously enhancing tumor invading the right portal vein and extending down to the confluence of right and left portal veins. The main and left portal veins are widely patent. Diagnosis: Hepatoma with invasion of right portal vein. Submitted by Martin R. Prince, M.D., Ph.D., Ann Arbor, MI.
MIP of Entire 3D Volume Sub-Volume MIP Main Portal Vein SMV Main Portal Vein Axial Reformation
MIP of Entire 3D Volume Sub-Volume MIP Right Hepatic vein Right Hepatic vein Axial Reformation
55 year old female prior to TIPS Coronal 3D Gd MRA MIP during venous phase
Varices Thick MIP Thin MIP
Spleno-renal shunt Anterior MIP Posterior MIP
Fig. 7.3. MRA of Portocaval Shunt. Clinical Scenario: 42-year-old male, status post-portocaval shunt with worsening ascites. Technique: Coronal Acquisition, TR/TE/Flip = 7.2/1.2/45°, Field-of-View = 300 x 300, Matrix = 256 x 128, Centric Ordering of k-space, Acquisition Time = 32 s, 1 NEX, 40 ml of gadolinium infused at 2 ml/s, and timed empirically. Interpretation: Coronal subvolume MIP (a) and magnification view (b) shows a widely patent portocaval shunt (arrows). Note also gastric varices (arrowheads). During this equilibrium phase image, there is comparable enhancement of the portal vein, IVC, and aorta. Diagnosis: Patent portocaval shunt. Submitted by David Stafford-Johnson, M.D., Ann Arbor, MI. Reprinted with permission from Investigative Radiology Sept. Oct. 1998.
56 year old female with abdominal pain Minimun intensity projections Maximum intensity projection
Portal and hepatic vein thrombosus Minimun intensity projections Maximum intensity projection
Acute thrombosis of portal vein (arrows) with perithrombus enhancement (arrowheads) Maximum Intensity Projection
Fig. 7.4. Liver Transplant. Clinical Scenario: Status post liver transplant with increased liver function tests. Technique: Coronal Acquisition, TR/TE/Flip = 7/2.1/45°, Field-of-View = 320 x 320 x 84 mm, Matrix = 256 x 128 x 28, Sequential Ordering of k-space, Acquisition Time = 27 s, 40 ml gadolinium contrast infused at 2 ml/ s, and timed empirically. Interpretation: Coronal oblique subvolume MIP shows a widely patent splenic and portal veins. There is minor narrowing (arrows) at the site of anastomosis between the native and donor portal veins. Diagnosis: Widely patent transplant portal vein. Submitted by Martin R. Prince, M.D., Ph.D., Ann Arbor, MI. v
13 year old female post liver and kidney transplant Portal-venous Phase Arterial Phase
Post Liver Transplant with abcess narrowing portal vein
Pancreatic mass encasing celiac and spleno-portal confluence
Summary • Normal flow: Gd not necessary • Slow flow: Gd essential • Coronal 3D: thick slices & breathholding • Useful for evaluating • Varices • Shunts • Tumor encasement • Tumor invasion • Thrombosis • Cavernous transformation • Budd Chiari • Liver transplant