Download
1 / 42
500 likes | 910 Views
Anesthetic Implications of Pheochromocytoma & Cushing syndrome &Addison’s disease. Moderator-Dr Jyoti Pathania Presented by-Dr Kamal Prakash Sharma. Pheochromocytoma. 0.01-0.1% of HTN population Found in 0.5% of those screened M = F 3 rd to 5 th decades of life

E N D
Anesthetic Implications of Pheochromocytoma & Cushing syndrome &Addison’s disease Moderator-Dr Jyoti Pathania Presented by-Dr Kamal Prakash Sharma
Pheochromocytoma • 0.01-0.1% of HTN population • Found in 0.5% of those screened • M = F • 3rd to 5th decades of life • Rare, investigate only if clinically suspicion: • Signs or Symptoms • Severe HTN, HTN crisis • Refractory HTN (> 3 drugs) • HTN present @ age < 20 or > 50 ? • Adrenal lesion found on imaging (ex. Incidentaloma)
Pheo: Signs & Symptoms • The five P’s: • Pressure (HTN) 90% • Pain (Headache) 80% • Perspiration 71% • Palpitation 64% • Pallor 42% • Paroxysms (the sixth P!) • The Classical Triad: • Pain (Headache), Perspiration, Palpitations • Lack of all 3 virtually excluded diagnosis of pheo in a series of > 21,0000 patients
Pheo: Paroxysms, ‘Spells’ • 10-60 min duration • Frequency: daily to monthly • Spontaneous • Precipitated: • Diagnostic procedures, I.A. Contrast (I.V. is OK) • Drugs (opiods, unopposed -blockade, anesthesia induction, histamine, ACTH, glucagon, metoclopramide) • Strenuous exercise, movement that increases intra-abdo pressure (lifting, straining)
Pheo: Hypotension! • Hypotension (orthostatic/paroxysmal) occurs in many patients • Mechanisms: • ECFv contraction • Loss of postural reflexes due to prolonged catecholamine stimulation • Tumor release of adrenomedullin (vasodilatory neuropeptide)
Pheo: Signs & Symptoms • N/V, abdo pain, severe constipation (megacolon) • Chest-pains • Anxiety • Angina/MI with normal coronaries: • Catecholamine induced: myocardial oxygen consumption or coronary vasospasm • CHF • HTN hypertrophic cardiomyopathy diastolic dysfn. • Catechols induce dilated cardiomyopathy systolic dysfn. • Cardiac dysrhythmia & conduction defects
Pheo: Signs (metabolic) • Hypercalcemia • Associated MEN2 HPT • PTHrP secretion by pheo • Mild glucose intolerance • Lipolysis • Weight-loss • Ketosis > VLDL synthesis (TG)
Pheo: ‘Rule of 10’ • 10% extra-adrenal • 10% occur in children • 10% familial • 10% bilateral or multiple (more if familial) • 10% recur (more if extra-adrenal) • 10% malignant • 10% discovered incidentally
Catecholamines Metabolites MAO, COMT TH Tyrosine L-Dopa Dopamine Homovanillic acid (HVA) DBH COMT Norepinephrine Normetanephrine PNMT MAO COMT Epinephrine Metaneprine MAO Vanillymandelic Acid (VMA)
Familial Pheo • MEN 2a • 50% Pheo (usually bilateral), MTC, HPT • MEN 2b • 50% Pheo (usually bilatl), MTC, mucosal neuroma, marfanoid habitus • Von Hippel-Landau • 50% Pheo (usually bilat), retinoblastoma, cerebellar hemangioma, nephroma, renal/pancreas cysts • NF1 (Von Recklinghausen's) • 2% Pheo (50% if NF-1 and HTN) • Café-au-lait spots, neurofibroma, optic glioma • Familial paraganglioma • Familial pheo & islet cell tumor • Other: Tuberous sclerosis, Sturge-Weber, ataxia-telangectgasia, Carney’s Triad (Pheo, Gastric Leiomyoma, Pulm chondroma)
24h Urine Collection • 24h urine collection: • Creatinine, catecholamines, metanephrines, vanillymandelic acid (VMA), +/-dopamine • HPLC with electrochemical detection or mass spect • Positive results (> 2-3 fold elevation): • 24h Ucatechols > 2-fold elevation • ULN for total catechols 591-890 nmol/d • 24h Utotal metanephrines > 1.2 ug/d (6.5 umol/d) • 24h UVMA > 3-fold elevation • ULN 35 umol/d for most assays Sensitivity increased if 24h urine collection begun at onset of a paroxysm
Plasma Catecholamines • Drawn with patient fasting, supine, with an indwelling catheter in place > 30 min • Plasma total catechols > (2000 pg/mL) • SEN 85% SPEC 80% • False positives: same as for 24h urine testing, also with diuretics, smoking • CRF & ESRD: • Oliguric to Anuric 24h Urines inaccurate • Plasma epinephrine best test for pheo in ESRD • Plasma norepi and metanephrines falsely elevated in ESRD
Plasma Metanephrines • Not postural dependent: can draw normally • Secreted continuously by pheo • SEN 99% SPEC 89% • False Positive: acetaminophen • Assay not readily available in Canada
Suppression/Stimulation Testing • Clonidine suppression • May precipitate hypotensive shock! • Unlike normals, pheo patients won’t suppress their plasma norepi with clonidine • Glucagon stimulation • May precipitate hypertensive crisis! • Pheo patients, but not normals, will have a > 3x increase in plasma norepi with glucagon
Localization: Imaging • CT abdomen • Adrenal pheo SEN 93-100% • Extra-adrenal pheo SEN 90% • MRI • > SEN than CT for extra-adrenal pheo • MIBG Scan • SEN 77-90% SPEC 95-100% • 111Indium-pentreotide • Some pheo have somatostatin receptors • PET • 18F-fluorodeoxyglucose (FDG) • 6-[18F]-fluorodopamine
Pheo Management • Prior to 1951, reported mortality for excision of pheochromoyctoma 24 - 50 % • HTN crisis, arrhythmia, MI, stroke • Hypotensive shock • Currently, mortality:0 - 2.7 % • Preoperative preperation, -blockade? • New anesthetic techniques? • Anesthetic agents • Intraoperative monitoring: arterial line, EKG monitor, CVP line, Swan-Ganz • Experienced & Coordinated team: • Endocrinologist, Anesthesiologist and Surgeon
Preoperative Workup • CBC, Electroytes, creatinine, INR/PTT • FBS • Ca (if one of MEN syndrome is suspected) • CXR • EKG • Echo (r/o dilated CMY 2º catechols)
Preop Preperation Regimens • Combined + blockade • Phenoxybenzamine • Selective 1-blocker (ex. Prazosin) • Propanolol • Metyrosine • Calcium Channel Blocker (CCB) • Nicardipine • No Randomized Clinical Trials to compare various regimens!
Preop: + blockade • Start at least 10-14d preop • Allow sufficient time for ECFv re-expansion • Phenoxybenzamine • Drug of choice (noncompetitive & long acting) • Covalently binds -receptors (1 > 2) • Start 10 mg po bid increase q2d by 10 mg/d • Maintenance 40-80 mg/d (some need > 200 mg/d) • End points indicating adequate preop preparation are- 1) Increase until BP control and no more paroxysms ,no in hospital BP higher than 165/90 should be evident for 48 hours before surgery 2) FBS will return to normal 3) PCV will decline to around 40-43% 4) Orthostatic hypotension should be present, but BP on standing mg/d)should not be lower than 80/45 mm of Hg 5) ECG must be free of ST-T changes that are not permanent 6) No > 1 premature ventricular contraction should occur every 5 minutes
Preop: + blockade • Phenoxybenzamine (cont’d) • Side-effect: orthostasis with dosage required to normalized seated BP, reflex tachycardia • Drawback: periop hypotension/shock unlikely to respond to pressor agent. • Selective 1-blockers • Prazosin, Terazosin, Doxazosin • Some experience with Prazosin for Pheo preop prep • Not routinely used as incomplete-blockade • Less orthostasis & reflex tachycardia then phenoxybenzamine • Used more for long-term Rx (inoperable or malignant pheo)
Preop: + blockade • -blockade Used to control reflex tachycardia and prophylaxis against arrhythmia during surgery • Start only after effective -blockade (may ppt HTN) • If suspect CHF/dilated CMY start low dose • Propanolol most studied in pheo prep • Start 10 mg po bid increase to cntrl HR
Preop: + blockade • If BP still not cntrl despite + blockade • Add Prazosin to Phenoxybenzamine • Add CCB, ACE-I • Avoid diuretics as already ECFv contracted • Metyrosine
Preop: + blockade • Medications given on Morning of surgery • Periop HTN: • 1) IV phentolamine • Short acting non-selective -blocker • 2) IV Nitroprusside (NTP) • Periop arrhythmia: IV esmolol • Periop Hypothension: IV crystalloid +/- colloid
Pheo: Rx of HTN Crisis • IV phentolamine • IV NTP • IV esmolol • IV labetalol – combined + blocker
Preop: Metyrosine TH Tyrosine L-Dopa Dopamine • Synthetic inhibitor of Tyrosine Hydroxylase (TH) • Start 250 mg qid max 1 gm qid S/E’s: sedation, extra pyramidal, diarrhea,, anxiety, renal/cholelithiasis, galactorrhea N/V • Alone may insufficiently control BP and reported HTN crises during operation • Restrict use to inoperable/malignant phaeochromocytoma or as adjunct to + blockade or other preoperative prep DBH Norepinephrine PNMT Epinephrine
Preop: CCB • Nicardipine Block norepi mediated ca uptake into vascular smooth muscles • Started po 24h to few weeks preop to control BP and allow ECFv restoration • After intubation IV Nicardipine (start 2.5 ug/kg/min) • IV Nicardipine adjusted to SBP • Stopped prior to ligation of tumor venous drainage • Tachycardia Rx with concurrent IV esmolol • Advantage: periop hypotension may still respond to presser agents as opposed to those patients who are completely -blocked
Perioperative • Admit night before for overnight IV saline • 2 large bore I/V lines should be secured • Arterial line • CVP line • Routine Pulse oximetry,etCO2,EKG,Temperature probe • Known CHF: consider Swan-Ganz • Regardless of preop medications: • Have ready: IV phentolamine, IV NTP, IV esmolol • Rx hypotension with crystalloid +/- colloid 1st • Aim for CVP 12 or Wedge 15 • Inotropes may not work!
Intraoperative considerations Three critical phases of tumor resection are 1) Induction and intubation 2) Surgical manipulation 3) After ligation of the tumors venous drainage
Induction & Intubation • Etomidate, thiopental, and propofol can all be used to initiate anesthesia. • Increase anesthetic depth by bag mask ventilation with volatile anesthetic • Lidocaine 1-2mg/kg 1 min prior to induction • Narcotics • Fast acting antihypertensive readily available • Anesthetic choice: • En/Sevo/isoflurane: don’t sensitized myocardium to catecholamines • Halothane: may sensitize heart arrhythmia
Maintenance(During surgery) • Anesthesia is maintained with gases and narcotics. VA are easy to titrate, can help with HTN (1.5-2 MAC) • Pt should be kept normovolemic. • Blood glucose monitoring • Hypertensive episodes managed by- • Deepening volatile anesthetic level • Nitroprusside @ 0.5-10ugm/kg/m via infusion • Phentolamine mixed at 10mg/100ml D 5W(tachycardia can occur,small dose of esmolol/propranolol can treat it)
Maintenance(During surgery) • Propranolol/Short acting beta blocker Esmolol may be required during this period if there is persistent tachycardia/premature ventricular contractions
Ligation of the tumors venous drainage • ↓ circulating catecholamine causing hypotension • After ligation of all venous drainage arterial pressure commonly declines r/t ↑CO, ↓ SVR Treatment • ↓ VA • ↑ IVF • Phenylephrine or nor epinephrine
Postop • 1) Invasive lines should stay intact. Pt still at risk for liable BP. • 2) Pt susceptible to hypotension that is refractory to fluid volume expansion • 3) Still have high volumes of circulating catecholamine despite tumor resection • 4) Catecholamine levels normalize after several days. 75% of pts BP returns to normal after 10 days • 5) Prone to Hypoglycemia. Secondary to suppression of β-cell function disappears after the tumor is removed
Pheo & Pregnancy • Diagnosis with 24h urine collections and MRI • No stimulation tests, no MIBG if pregnant • 1st & 2nd trimester (< 24 weeks): • Phenoxybenzamine + blocker prep • Resect tumor laprascopically • 3rd trimester: • Phenoxybenzamine + blocker prep • When fetus large enough: cesarian section followed by tumor resection
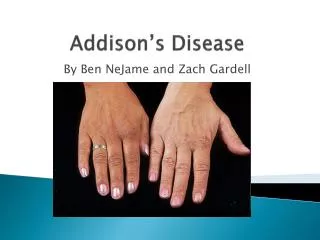
Addison's disease • Addison's disease is characterized by decreased or absent glucocorticoid secretion, usually combined with mineralocorticoid insufficiency. It can be primary or secondary and may present as an acute, chronic, or acute-on-chronic illness. The most common cause is autoimmune. A) Clinical features • Postural hypotension & dizziness • Hyperkalemia & Hyponatremia Hypoglycemia Nausea, vomiting, diarrhea, and weight loss. Decreased body hair. Pigmentation especially in areas exposed to the sun. Can be associated with pernicious anemia, myasthenia gravis, and vitiligo May not be clinically obvious until a significant stress occurs B) Investigations- 1) Low serum glucose. 2) Low Na+, raised K+ and urea 3) Low Bicarbonates,Nomocytic anemia
4) Plasma ACTH-measure simultaneously with plasma cortisol at 08:00h. Even if cortisol is normal the ACTH will be elevated. 5) Plasma renin activity and aldosterone—plasma renin activity is usually low with a low aldosterone. 6) Short Synacthen(Cosyntropin) stimulation test—250 µg of Synacthen dissolved in 1 ml of sterile water is given i/v or i/m. Serum cortisol is measured 30-60 min later. A serum cortisol >495 nmol/litre excludes the diagnosis. C) Management- • 1) Hydrocortisone 200 mg IV should be given immediately, then 100 mg 6-hourly IM or 200 mg/24 h IV, until oral replacement is possible(Hydrocortisone orally: 20 mg in the morning and 10 mg at night) • 2) Fludrocortisones to replace aldosterone:0.05- 0.1 mg daily orally. • 3) To maintain NaCl daily intake to 3-4gm/d • 4) Fluid resuscitation with CVP guidance. 0.9% saline is an appropriate fluid with 50% dextrose infused if hypoglycaemia occurs. • 5) Inotropes if hypotension persists. The choice of inotrope will depend on the clinical picture, i.e. noradrenaline if the patient has severe vasodilatation.
Perioperative management of patients with Addison's disease 1)Give all medication up to the morning of surgery. 2)25 mg IV hydrocortisone should be given at induction. 3)Small or intermediate cases should be managed as per perioperative steroids 4)In major cases, hydrocortisone 200 mg/24 h should be used until the patient can be weaned back onto maintenance therapy. 5) Blood glucose and electrolytes. POSTOPERATIVELY- • To continue Hydrocortisone I/v until oral maintenance dose is started • To start fludrocortisone 0.05-0.1 mg/d • Monitor Blood glucose • Monitor daily electrolytes
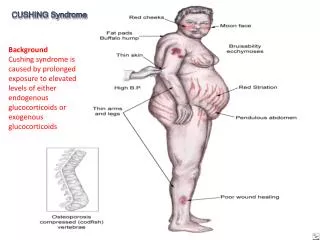
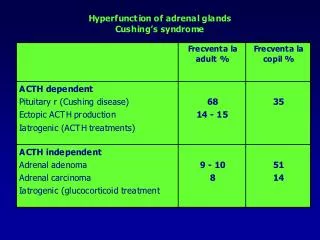
Cushing's syndrome Cushing's syndrome is a collection of signs and symptoms due to an excessively high plasma cortisol. The most common cause of Cushing's syndrome is treatment with glucocorticoid drugs. Anesthetists will see this syndrome in: 1) Patients having pituitary or adrenal surgery to resects tumors causing a raised cortisol. 2) Patients with malignant tumors. These occasionally secrete an ACTH-like hormone that causes profound Cushinoid features. Oat cell carcinoma of the lung is a common cause. 3) Patients on high-dose steroid therapy. Clinical features- Moon face and truncal obesity. Proximal myopathy and osteoporosis. Easy bruising and fragile skin. Impaired glucose tolerance, diabetes. Hypertension and left ventricular hypertrophy. Hypernatremia and hypokalaemia. Gastrointestinal reflux & Sleep apnea.
Diagnosis 1)Classical clinical features are often seen but will not differentiate the various causes of a raised cortisol level. Urinary free cortisol or lack of diurnal variation will confirm a pathological cause but will not define the etiology. 2)The ‘short dexamethasone suppression test’ (1 mg of dexamethasone is given at night and a cortisol sample taken in the morning) is a sensitive test to confirm abnormally raised serum cortisol. Serum cortisol will be suppressed in the morning if the HPA axis is working normally. 3)Serum ACTH levels will help determine if adrenal or pituitary pathology is the cause. 4)Very high ACTH levels suggest ectopic production, e.g. carcinoma of the lung, and very low levels suggest adrenal hyper secretion. 5)The ‘high dose dexamethasone suppression test’ (2 mg is given 6-hourly for 48 h and serum cortisol measured) will cause a fall in early morning and urinary free cortisol on the second day in pituitary-dependent Cushing's syndrome, but not in ectopic or adrenal causes. 6)Inferior petrosal venous sinus sampling following CRH stimulation is the final confirmatory test for pituitary Cushing's syndrome. 7)MRI scan of the pituitary fossa.
Treatment of cushing syndrome • 1) Selective Transsphenoidal resection is treatment of choice for Cushing disease(Pituitary micro/macroadenoma) • 2) Adrenalectomy uni/bilateral needed( for adrenal adenoma/carcinoma) • 3) Pt will be medically treated prior to surgery with focus on decreasing synthesis of steroids by -Aminoglutethimide,Ketoconazole -Mitotane -Metyrapone & Cyproheptadine • 4) Spirinolactone to control BP & restore electrolyte balance may be needed • 5) Insulin to control plasma glucose levels may be required • 6) All above measures contd. to the day of surgery
Preoperative assessment 1) 85% of patients are hypertensive and are often poorly controlled. 2) ECG abnormalities (high-voltage QRS and inverted T waves) can make IHD difficult to exclude but will revert to normal after curative surgery. These ECG changes seem to be related to the Cushing's disease itself. 3) 60% of patients have diabetes or impaired glucose tolerance and a sliding scale should be started before major surgery if glucose is >10 mmol. 4) Gastroesophageal reflux is common and preoperative acid suppression therapy and rapid sequence induction should be considered. 5)Venous access can be very difficult. 6) Patients can be obese and appropriately sized blood pressure cuffs, operating tables, and supports should be ordered. INTRAOPERATIVELY- • 1) Careful positioning of pt because of osteoporosis • 2) Despite routine monitoring CVP is monitored as these pt tend to have higher CVP • 3) Adequate control of blood sugar • 4) We normally begin administering glucocorticoids at the start of resectioning of tumor @ 100 mg of Hydrocortisone hemi succinate/phosphate i/v
POSTOPERATIVELY- • 1) Hydrocortisone @ 100 mg/24 hr is contd. i/v on the day of surgery & reduced over a period of 3-6 days until maintenance dose is reached • 2 )Beginning on the day 3rd a mineralocorticoid fludrocortisone @ 0.05-0.1mg/day orally started