Download
1 / 47
470 likes | 484 Views
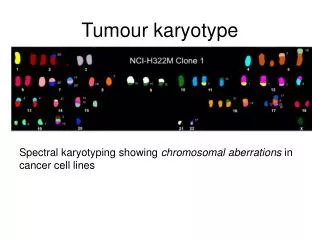
Tumour immunology. Tumor antigens. Tumor – specific antigens (TSA) complexes of MHC gp I with abnormal fragments of cellular proteins (chemically induced tumors, leukemia with chromosomal translocation)

E N D
Tumor antigens • Tumor – specific antigens (TSA) • complexes of MHCgp I with abnormal fragments of cellular proteins (chemically induced tumors, leukemia with chromosomal translocation) • complexes of MHCgp with fragments of oncogenic viruses proteins (tumors caused by viruses: EBV, SV40, polyomavirus…) • abnormal forms of glycoproteins (sialylation of surface proteins of tumor cells) • idiotypes of myeloma and lymphoma (clonotyping TCR and BCR)
Tumor antigens b) Tumor - associatedantigens (TAA) • presentalso on normalcells • differences in quantity, timeandlocalexpression • auxiliarydiagnosticmarkers
Tumor - associated antigens • onkofetal antigens -on normal embryonic cells and some tumor cells • -fetoprotein (AFP) - hepatom • carcinoembryonic antigen (CEA) - colon cancer • melanoma antigens - MAGE-1, Melan-A • antigen HER2/neu -receptor for epithelial growth factor, mammary carcinoma • EPCAM – epithelial cell adhesion molecule, metastases • differentiation antigens of leukemic cells - present on normal cells of leukocytes linage • CALLA -acute lymphoblastic leukemia (CD10 pre-B cells)
Anti-tumor immune mechanisms Immunecontrol • tumor cellsnormallyarise in tissues and are eliminated by Tcells
Anti – tumor immune response • tumor cells are weakly immunogenic • occurs when tumor antigens are presented to T cells by dendritic cells activated in the inflammatory environment
Regulatory T cells prevents removal of cancer cells and thus contribute to the development of the tumor.
Anti-tumor immune mechanisms If tumor cells are detected, in defense maybeinvolvednon-specificmechanisms(neutrophilicgranulocytes, macrophages, NK cells, complement) andantigen-specificmechanisms(TH1 and TC cells, antibodies).
Anti-tumor immune mechanisms • DC are necessary for activation of antigen specific mechanisms • predominance of TH1(IFN g, TNFa) • specific cell-mediated cytotoxic reactivity –TC • activation of TH2 → stimulation of B cells→ tumor specific antibodies production (involved in the ADCC) • tumor cells are destroyed by cytotoxic NK cells (ADCC) • interferons - antiproliferative, cytotoxic effect on tumor cells - INFg - DC maturation
Mechanisms of tumor resistance to the immune system • high variability of tumor cells • lowexpressionof tumor antigens • sialylation • someanticancersubstanceshave a stimulatingeffect • productionoffactorsinactivating T lymphocytes • expressionofFasL → T lymphocyteapoptosis • inhibitionofthefunctionordurabilitydendriticcells (NO, IL-10, TGF-b)
Transplantation = transfer oftissueor organ • autologous - donor = recipient • syngeneic- geneticallyidentical donor and recipient (identicaltwins) • allogeneic - geneticallynonidentical donor ofthesame species • xenogenic - the donor ofanother species • implant - artificialtissuecompensation
Allotransplantation • differences in donor-recipient MHC gp and secondary histocompatibility Ag • alloreactivity of T lymphocytes - the risk of rejection and graft-versus-host disease
Tests prior to transplantation • ABO compatibility (matching blood group) -risk of hyperacute or accelerated rejection (= formation of Ab against A or B Ag on graft vascular endothelium) • HLA typing (matching tissue type)-determining of HLA alelic forms by phenotyping or genotyping • Cross-match - detection of preformed alloantibodies • (after blood transfusions, transplantation, repeated childbirth) • Mixed lymphocyte reaction - testing of T lymphocytesalloreactivity
HLA typing 1) Serotyping (microlymfocytotoxic test)
HLA typing 2) Molecular genetic methods- genotyping 2a) PCR-SSP 2b) PCR-SSO 2c) PCR-SBT
Tests prior to transplantation Cross-match testing • determination of preformed alloantibodies • recipient serum + donor lymphocytes + rabbit complement → if cytotoxic Ab against donor HLA Ag are present in recipient serum , Ab activate complement → lysis of donor lymphocytes. Dye penetration into lysis cells. • positive test = the presence of preformed Ab → risk of hyperacute • rejection! → contraindication to transplantation
Tests prior to transplantation Mixed lymphocyte reaction (MRL) • determination of T lymphocytesalloreactivity • mixed donor and recipient lymphocytes → T lymphocytes after recognition of allogeneic MHC gp activate and proliferate • One-way MRL • determination of recipient T lymphocytesreactivity against donor cells • donor cells treated with chemotherapy or irradiated lose the ability of proliferation
Rejection • hyperacute • accelerated • acute • chronic
Hyperacute rejection • minutes to hours after transplantation • humoral mediated immune response • mechanism: • if in recipients blood are present preformed or natural Ab(IgM anti- carbohydrate Ag) before transplantation→ Ab + Ag of graft (MHC gp or endothelial Ag) → graft damage by activated complement • the graft endothelium: activation of coagulation factors and platelets, formation thrombi, accumulation of neutrophil granulocytes • prevention: • negative cross match before transplantation, ABO compatibility
Acceleratedrejection • 3 to 5 daysaftertransplantation • caused by antibodiesthat don´t activatecomplement • cytotoxicandinflammatoryresponsestriggered by bindingofantibodies to Fc-receptors on phagocytesand NK cells • prevention: • negative crossmatchbeforetransplantation, ABOcompatibility
Acute rejection • days to weeks after the transplantation or after a lack of immunosuppressive treatment • cell-mediated immune response • mechanism: • reaction of recipient TH1 and TC cells against Ag of graft tissue • infiltration by lymphocytes, monocytes, granulocytes around smallvessels → destruction of tissue transplant
Chronic rejection • from 2 months after transplantation • the most common cause of graft failure • mechanism is not fully understood: • non-immunological factors (tissue ischemia) and TH2 response with production alloantibodies, pathogenetic role of cytokines and growth factors (TGFβ) • fibrosis of the internal blood vessels of the transplanted tissue, endothelial damage →impaired perfusion of graft → gradual loss of its function • dominating findings: vascular damage
Rejection • Factors: • Thegeneticdifferencebetween donor and recipient, especially in thegenescodingfor MHC gp (HLA) • Type oftissue / organ - thestrongestreactionsagainstvascularizedtissuescontaining many APC (skin) • Theactivityofthe recipientimmunesystem – theimmunodeficiency recipient has a smallerrejectionreaction; immunosuppressivetherapyaftertransplantation – suppressionofrejection • Status oftransplanted organ - thelengthofischemia, themethodofpreservation, traumatization of organ at collection
Graft-versus-host (GvH) disease • after bone marrowtransplantation • GvHalsoafterbloodtransfusion to immunodeficiencyrecipients • T-lymphocytes in thegraft bone marrowrecognize recipient tissueAg as foreign (alloreactivity)
AcuteGvHdisease • days to weeksafterthetransplantationof stem cells • damageof liver, skin andintestinalmucosa • prevention: appropriate donor selection, theremovalof T lymphocytesfromthegraftandeffectiveimmunosuppression
Chonic GvH disease • months to years after transplantation • infiltration of tissues and organs by TH2 lymphocytes, production of alloantibodies and cytokines → fibrosis • process like autoimmune disease: vasculitis, scleroderma, sicca-syndrome • chronic inflammation of blood vessels, skin, internal organs and glands, which leads to fibrosis, blood circulation disorders and loss of function
Graft versus leukemia effect (GvL) • donor T lymphocytes react against residual leukemick cells of recipient (setpoint response) • mechanism is consistent with acute GvH • associated with a certain degree of GvH (adverse reactions)
Immunopathological reactions • Immune response which caused damage to the body (Consequence of immune response against pathogens, inappropriate responses to harmless antigens; autoimmunity)
Immunopathological reactions Classification by Coombs and Gell Immunopathological reactions: immune response, which caused damage to the body (secondary consequence of defense responses against pathogens, inappropriate responses to harmless antigens, autoimmunity) IV types of immunopathological reactions: Type I reaction - response based on IgE antibodies Type II reaction - response based on antibodies, IgG and IgM Type III reaction- response based on the formation of immune complexes Type IV reaction - cell-mediated response
Immunopathologicalreactionsbased on antibodiesIgGandIgM (reaction type II) CytotoxicantibodiesIgGandIgMbind to antigens on own cell: • complementactivation • binding to Fcreceptors on phagocytesand NK cells (ADCC)
Examples of immunopathological reaction Type II • Transfusionreactionsafteradministrationofincompatibileblood: bindingofantibodies to antigens on erythrocytes → activationoftheclassicalpathwayofcomplement → cell lysis • Hemolyticdiseaseofnewborns: caused by antibodiesagainstRhD antigen
Examples of immunopathological reaction Type II Autoimmune diseases: • organ-specific cytotoxic antibodies (antibodies against erythrocytes, neutrophils, thrombocytes, glomerular basement membrane ...) • blocking or stimulating antibodies Graves - Basedow's disease - stimulating antibodies against the receptor for TSH Myasthenia gravis - blocking of acetylcholin receptor→ blocking of neuromuscular transmission Pernicious anemia - blocking the absorption of vitamin B12 Antiphospholipid syndrome - antibodies against fosfolipids Fertility disorder - antibodies against sperms or oocytes
Immunopathological reactions based on immune complexes formation (reaction type III) • caused by IgG antibodies → bind to antigen → creation of immune complexes • immunocomplexes - bind to Fc receptors on phagocytes • - activate complement • immune complexes, depending on the quantity and structure, are eliminated by phagocytes or stored in tissues
Immunopathological reactions type III • pathological immunocomplexes response arises when is a large dose of antigen, or antigen in the body remains; arise 10-14 days after aplication of Ag and induced inflamation (can get to chronic state) • immune complexes are deposited in the kidneys (glomerulonephritis), on the surface of endothelial cells (vasculitis) and in synovie joint (arthritis)
Serum sickness • the therapeutic application of xenogeneic serum (antiserum to snake venom) • creation of immune complexes and their storage in the vessel walls of different organs • clinical manifestations: urticaria, arthralgia, myalgia • Systemic lupus erythematosus • antibodies against nuclear antigens, ANA, anti-dsDNA • Farmer's lung • IgG antibody against inhaled antigens (molds, hay) • Post-streptococcal glomerulonephritis, cryoglobulinemia, revmatoid arthritis, post-infectious arthritis
Immunopathological delayed-type reaction (reaction type IV) • delayed-type hypersensitivity (DTH) • local reaction caused by TH1 cells and monocytes / macrophages (physiologically – elimination of macrophage intracellular parasites) • immunization by antigen → formation of antigen specific TH1 cells (and memory cells) • 12-48 hours after next contact with antigen arise local reaction – granuloma(TH1and macrophage infiltration) • Tuberculin reaction • Tissue damage in tuberculosis and leprosy • Sarcoidosis • Multiple sclerosis
Subtype IV - Cellular cytotoxic response(Tc activation) similar to DTH reaction TH1 cells activate CD8 + T lymphocytes viral rashes viral hepatitis acute rejection of transplanted organ some autoimmune thyroiditis contact dermatitis
Contact dermatitis • is a localized rash or irritation of the skin caused by contact with alergen (nickel , chromium, ingredients in cosmetic products , plant allergens and other) • the first is senzitization • appears in 24 – 48 hours after second contact with alergen • diagnosis : patch test
Patch test patch test is a method used to determineif a specific substance causes allergic inflamation of the skin Allergens are applied to special hypoallergenic patch on the back skin Results are evaluated after 48 and 72 hours In positive reactionappearseczema
Tumour immunology and immunotherapy • https://www.youtube.com/watch?v=K09xzIQ8zsg • This is how your immune system fights cancer • https://www.youtube.com/watch?v=UM2f-qFZV3o