Download
1 / 46
470 likes | 752 Views
Health Economics Facts and Practice in Jordan Dr. AbdelRazzaq Shafei MOH - Community Health Consultant April 2019 Balqa Applied University. Health economics - Definition

E N D
Health Economics Facts and Practice in JordanDr.AbdelRazzaq ShafeiMOH- Community Health ConsultantApril 2019Balqa Applied University
Health economics - Definition Health economics is a branch of economics concerned with issues related to efficiency, effectiveness, value and behavior in the production and consumption of health and healthcare. In broad terms, health economists study the functioning of healthcare systems and health-affecting behaviors such as smoking.https://en.wikipedia.org/wiki/Health_economics
Health economics from WHO worksCost effectiveness and strategic planning (WHO-CHOICE) WHO-CHOICE is a program in the World Health Organization that helps countries decide health system priorities based on considerations of costs and impacts. A number of different methods and tools contribute to the program of work: The Generalized Cost-Effectiveness component of the program is interested in identifying health care interventions that provide the greatest value for money – the largest health gain for each dollar spent on health. The OneHealth Toolis used to help countries to examine the costs and feasibility of their strategic plans, as well as to evaluate the potential impact of the plan.
Continued………… WHO-CHOICE data and methodology has been used in the calculation of “Global Price Tags”, estimating resource requirements for scaling up health care interventions for specific disease areas across countries. WHO-CHOICE supports the use of Geographic Information Systems (GIS)to analyze physical accessibility to health services, linking the results to national planning and costing processes, and policy discussions on how to optimize investments in the health system. Recognizing that the consequences of disease and injury reach beyond health, WHO-CHOICE provides guidance and a framework for evaluating the economic consequences of disease and injury.
continued OneHealth Tool The tool provides planners with a single framework for scenario analysis, costing, health impact analysis, budgeting and financing of strategies for all major diseases and health system components. It is thus primarily intended to inform sector wide national strategic health plans and policies. Outputs from an application will help planners answer the following questions: What would be the health system resources needed to implement the strategic health plan (e.g., number of nurses and doctors required over the next 5-10 years)? How much would the strategic plan cost, by year and by input? What is the estimated health impact? How do costs compare with estimated available financing?
Health economics from USAID works Health economics is concerned with the alternative uses of resources in the health services sector and with the efficient utilization of economic resources such as Human resource, material and financial resources. Every health worker needs to acquaint him/ her self with the basic concepts of economics and its application to the health sector in order to manage health institutions and health delivery system efficiently. “Health economics” as a course is meant to give medical, health officer and other paramedical students basic principles regarding economics and its application to the health sector.
Health economics applicationsin developing countries The concept of health human capital guides the statistical study of (1) health production functions (2) derived demands for medical and behavioral health inputs (3) determinants of health and productivity outcomes
CDC- Centers for Disease Control and Prevention Public Health Economics and Methods Economics is the study of decisions—the incentives that lead to them, and the consequences from them—as they relate to production, distribution, and consumption of goods and services when resources are limited and have alternative uses. CDC uses economics to identify, measure, value, and compare the costs and consequences of alternative prevention strategies.
Health Economics in Jordan-Health economicdivision/directorate The concept of health economics:Health economics is a modern branch of economics, which examines how to apply the tools of economics to health care issues, and to clarify their different aspects, so that they are more susceptible to analysis. Economics also provides criteria for determining whether health policies increase or reduce economic efficiency and the equitable distribution of health care. Health economics is also concerned mainly with the allocation of scarce economic resources between competing health care uses, whose resources are scarce, while the need for them increases over
The economics of health answer three basic questions:- How much resources do the common -How is health care provided at the lowest possible cost?-How are health services distributed to those who need them fairly? • Health Economics in Jordan-Health economic division/directorate Continued
Objectives to be achieved:1) Disseminate the concept of health economics and its components among decision makers and health sector workers.2) to draw the attention of state officials on alternative ways to finance health services to ensure continuity of delivery, especially that the financing of health services in the Kingdom depends on about 50% of government funding.3) Emphasize the importance of health insurance with a focus on finding health insurance for the poor so as to ensure equitable access to health services. 4) control and contain the costs of providing health services, especially that the prices of health services are increasing at rates higher than the increase in prices of other goods and 5) Enhancing the role of the private sector in providing health care and encouraging investment in health services and privatization initiatives in the health sector to become a complementary role services around the world • Health Economics in Jordan-Health economic division/directorate Continued
Mechanisms to achieve the desired objectives in the field of health economics:1) The introduction of the subject of health economics in the curricula of higher education, especially in the faculties of medicine, health sciences and administrative sciences colleges.2) The implementation of research and studies that focus on the problem of financing health services on government funding, since this funding is not guaranteed to be based on relatively irregular revenues and the application of other financing alternatives such as private sector financing and non-profit institutions. 3)To require the implementation of health insurance for non-Jordanians in accordance with the civil health insurance system, with emphasis on the provision of health insurance to the poor who are unable to pay.4) Issuance of regulations and regulations that oblige government agencies providing health services with lists of cost analysis of services provided, cost and benefit analysis, national health accounts and feasibility studies of health projects before financing them.5) Develop regulations and laws that encourage investment in health services and support public-private partnership in health care delivery • Health Economics in Jordan-Health economic division/directorate Continued
Health Economics in Jordan-Health economic division/directorate Continued Directorate mission • Enhancing and supporting the Ministry of Health's own capacity to use the concept of health economics and its analytical tools in decision-making, whether at the managerial level or the level of health policies.
Health Economics in Jordan-Health economic division/directorate Continued General goals 1) Enhance the capacity of practical health personnel to use the means and tools of the health economy to develop health care policies, planning and resource allocation. 2)Strengthen national research capacities in the health economy to increase efficiency and efficiency and equity in the delivery of health services 3)Strengthening and supporting the Ministry of Health's own capacities through the following main activities. 4)Work on developing the expertise of scientific and practical health personnel in the optimal use of resources. 5)Providing advice on health economics topics through field studies and economic research.
Health Economics in Jordan-Health economic division/directorate Continued General goals 6) Participation with the relevant administrative units in the Ministry of Health such as planning, project management and health insurance in prioritizing health programs.7)Support and promote the restructuring of the health sector.8)Follow-up and analysis of the aspects of funding and health expenditure and the periodic identification of expenditure rates and their impact on the national health level.9)Conducting and analyzing the economic cost of health services.10)Development of cost containment mechanisms and alternatives in health services11)Contribute to improving the level of health care provided to citizens in cooperation with all relevant bodies and in all inputs of the health sector.
Departments of Health Economics - Department of Accounts and Health Financing.- Department of Health Economics Development.
Department of Accounts and Health Financing )main tasks) -Review public sector spending on the health sector.-Participate in budgeting for health programs and projects.-Participate in the distribution of the necessary allocations for programs included in the budget of the Ministry of Health.-Develop alternatives to sustainable health sector financing.-Compiling, compiling and analyzing data on health expenditure from all sectors, including health insurance funds in the public and private sectors.-Collection of economic and social indicators -Follow-up the development and modern methodologies used in the preparation of national health accounts and linking this with funding and spending.-Prepare periodic reports of national health accounts and develop appropriate policy interventions
Department of Health Economics Development )main tasks( -Calculation costs in the Ministry and comparing them with other health sectors.-Reduce waste and contain the cost of health services.-Participate in the expansion of health insurance umbrella.-Contribute to the development and promotion of pharmaceutical health policies-Include rational drug use and cost control.-Adopt expenditure-oriented spending policies
تعريف الحسابات الصحية الوطنية • تعتبر الحسابات الصحية الوطنية أداة لرسم السياسة الصحية و صناعة و اتخاذ القرارات كونها تشكل الإطار العــام لاحتساب إجمالي الإنفاق الصحـي على مستوى الدولة . • كما انها تعتبر أداة لوصف تدفق النفقات المالية في القطاع الصحي لسنة مالية محددة من خلال تحديد مصادر التمويل و تتبع التدفقات المالية لتحديد أوجه الصرف . • تعتبر الحسابات الصحية الوطنية منهجية عالمية موحدة معتمدة من قبل منظمة الصحة العالمية و البنك الدولي و الجهات الدولية الاخرى .
الحسابات الصحية الوطنية • تستخدم الحسابات الصحية الوطنية لتوفير مؤشرات الانفاق الصحي على المستوى الوطني وللإجابة وعلى عدة تساؤلات هامة و التي يطرحها صناع القرار و راسمي السياسات الصحية واصحاب القرار ومن ضمنها : • إجمالي حجم للإنفاق على القطاع الصحي . • نسبة إجمالي الإنفاق على القطاع الصحي من الناتج المحلي الإجمالي . • حصة الفرد من الانفاق على الصحة . • مصادر التمويل في القطاع الصحي (حكومي ، خاص، خارجي). • ما تم أنفاقه حسب برامج الرعاية الصحية ( الرعاية العلاجية، الرعاية الأولية ، الإدارة ، التدريب). • ما تم أنفاقه حسب البنود المحاسبية ( الرواتب ، الادوية ، الاجهزة و المعدات ، الانشاءات و غيرها من البنود).
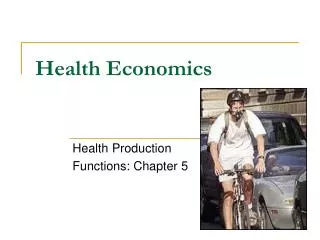
Jordanian Health Sector's Flow of Funds MOH/ CIP MOF MOH Facilities RMS / MIP RMS Facilities MOPIC UHs ( JUH – KAUH ) UHs (JUH – KAUH) Facilities Other Gov. Entities Other Gov. Entities Public Universities Universities Facilities Social Security Private Firms Private Facilities Private Insurance Enterprises Household Other Gov. Entities Facilities Household NGOs UNRWA NGOs Private Firms Private Universities UNRWA Clinics Rest of the world UNRWA
المصدر: دائرة الاحصاءات العامة ، التعداد العام للسكان و المساكن 2015
اجمالي الانفاق الصحي كنسبة من الناتج المحلي الاجمالي
حصة الفرد من الانفاق على الصحة بالدينار الاردني 2007 - 2015
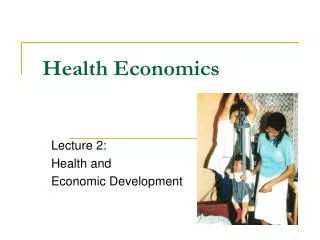
High Level National Consultation Workshop - Jordan National Health Sector Strategy and UHC, Amman-Jordan, 12 May 2015 Per Capita Total Health Expenditure, by Country Group, In Jordan, Total Health Expenditure per capita in 2015 US$ 333 /JD 236 Group 3 US$ 35–130 Group 2 US$ 150–600 Group 1 US$ 700–2000
The methodology of distribution total cost of hospitals to the hospital departments • Upon to the 3 hospitals cost studies 1-Implementing Hospital Autonomy in Jordan: Economic Analysis of Prince Raya Hospital (2002) 2- Implementing Hospital Autonomy in Jordan: Economic Analysis of Al-Karak Hospital (2002 3-Prince Hamza costing study (2007)
Continued We followed the same methodology mentioned in these 3 studies, but we followed the distribution of expenditure between departments on base of Prince Hamza hospital only because of: • Prince Hamza hospital study is more recent • The total cost of PrincesRaya hospital was less than 2 million and Alkarak hospital less than 3.5 JD million, which mean very low cost in comparison with recent costs, incomparison with Prince Hamza hospital which was about 17 million JD • The development of hospitals after 2000 • Nearly two-thirds of the hospitals total cost (variable and fixed) is consumed by centers directly engaged in the delivery of daily services.
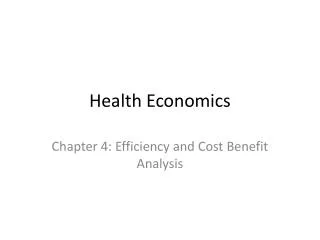
Continued -Outpatient clinics 20% -Emergency department 10% -ICU, CCU, P-ICU (pediatric) 11% -Inpatient departments 40% -Operating rooms 9% -Others services 10% (Daily cases, Hemodialysis, Dental department, Endoscopy)
Basic Methodology for these 3 hospitals With the oversight of the Hospital Decentralization Implementation Team and using a detailed list of all services offered by Al Karak hospital, Princes Raya hospital and Prince Hamza hospital, the hospital workgroups divided the services into two major “cost center” categories: Daily Hospital Services and Ancillary and Support Services. Once agreement was reached on the two broad classifications, the workgroups further divided the services into cost center subcategories. Under Daily Hospital Services, services that require similar labor and capital inputs and that treat patients with similar maladies were grouped into a single cost subcategory; those that require distinctly different inputs and treatment patterns were classified separately. Ancillary and Support Services comprises Administration/Finance, Rehabilitation, X-ray, Laboratory, Pharmacy, and Food and Beverage departments. As with Daily Hospital Services, cost center subcategories were determined based upon their inputs, as well as the outputs (services) that they perform in support of the hospital’s overall function.
Continued Once the cost centers were defined, the workgroups and Implementation Team created a detailed list of variable and fixed factors that the hospital utilizes. The variable factors, and the methodology employed to estimate these costs. (to follow)
Continued • Labor: This includes compensation paid to medical doctors, nurses/midwives, pharmacists, and administrative, finance, technical/medical, technical/nonmedical, and other personnel. An accurate list of employees who worked at the hospital was matched against MOH personnel records, which detailed the level of compensation for each employee.
Continued Non-labor Variable Factors: This variable input was divided into specific categories: utility inputs, structure and equipment inputs, consumable inputs, contracted services, and nonclinical supplies. Utility inputs include fuel, butane gas, telephone services, electricity, and water. Structure and equipment inputs include building renovations, rental unit for nurses’ quarters, building maintenance and renewal, equipment maintenance, and supplies. Consumable inputs include drugs and medications, gases, medical consumables, and laboratory and radiological consumables. Contracted services include food services, housekeeping services, laundry services, and other contracted services.
Continued • Nonclinical supplies include stationeries, textiles and linens, and perishables. • The allocation rule employed to distribute such costs across the various hospital cost centers. For example, butane gas use was distributed among cost centers according to the proportion of square meters of physical space that the cost center occupies, based on hospital blueprints and construction documents obtained from the MOH Department of Buildings.
Continued • The fixed factors and the methodology employed to estimate and distribute their costs among the cost centers. The fixed factors employed by these hospitals during the period of these studies. • Fixed Hospital Structure: the hospital building, electrical structures, sewage and plumbing structures, and CT-Scan facility • Hospital Vehicles: hearse, buses, sedans, ambulances, and pickup trucks • Equipment and Furniture: medical equipment and hospital furniture.
Distribution of total cost in Prince Hamza Hospital to the main departments
The methodology of distribution of total expenditure of MOH to the main tow programs of primary health care and curative care 1.Data collection :- Three types of data will be collected a. Financial data which include : - The total health expenditure of MOH level inside the ministry and its facilities from different resources ( MOF, health insurance, administration, grants and others )- Distribution of the total MOH expenditure by programs. - Distribution of the total MOH health expenditure by main services provided (mainly primary and secondary health care) - Allocation of secondary health care (hospitals) expenditure according to the previous cost study between departments (local and international studies). - The development of MOH and CHI budget at the least in the past 5 years. Main economic health indicators (per capita health expenditure, total health expenditure, public and private health expenditure … etc).
Continued b. Health service delivery data : Number of visits at the primary health care facilities (health centers). - Number of patients at the secondary health care facilities, (hospital by : - Inpatient. - Out patients. -Operations. -Emergency… etc. c. Demographic data: - Population - Ages distribution. - Insurance status. - Epidemiological for communicable and non communicable diseases, (if available). - Number of refugees … etc.
Continued 2- Validation of data and distribution of total MOH health expenditure to the output (service). 3- Analysis of data by using health statistics needed (averages, means .. etc)